





Preoperative airway assessment plays a key role in the context of difficult airway management. There is no general agreement that clarifies unambiguously and precisely how to conduct this assessment, and above all, which anatomical and physiological parameters must be taken into account for its correct execution. The American Society of Anesthesiologists (ASA) recommended conducting the preoperative assessment of the airways based on 11 anatomical variables, without hierarchising the various variables for effectiveness. The ASA states that the decision to evaluate only some or all the variables depends on the clinical context. Ultimately, the assessment remains at the discretion of the individual operator [1, 2]. Furthermore, in the literature there is no single parameter that is sufficiently valid to predict difficult endotracheal intubation [3–9]. Conversely, using composite predictive models, or by combining the different suggested parameters of difficult airways, the positive predictive value (PPV) or negative predictive value (NPV) of the evaluation increases [10–14]. A useful composite assessment tool for predicting difficult airways is the el-Ganzouri index (EL.GA) [11]. An anatomical parameter which currently is not usually evaluated for predictive purposes is the circumference of the neck. There is conflicting evidence in the literature concerning its usefulness in predicting possible difficult airways [15–17]. Moreover, there is no unanimous agreement on the cut-off above which the circumference of the neck could be predictive of difficult endotracheal intubation [17, 18].
From these premises, the aim of our retrospective observational study EL.GA+ is to validate the circumference of the neck, as an additional parameter to the EL.GA index (hence the choice of the acronym for the definition of the study: EL.GA+) in predictivity of airway management. We also aim to determine the cut-off above which the circumference of the neck correlates with difficult intubation.
METHODS
Study design and setting
This is a single-centre, retrospective, observational study conducted at the Department of General and Specialised Surgery of the academic hospital University of Campania “Luigi Vanvitelli” located in Naples, from November 2016 to May 2017.
Study population
After obtaining the local ethic committee approval on 22 November 2019, we analysed the records of 240 patients who had an elective surgical procedure, under general anaesthesia, requiring endotracheal intubation. Patients who had undergone other types of anaesthesia different from the general one, who had a documented history of difficult airways, who had abnormalities of the cervical spine and/or who had undergone emergency procedures were excluded.
Conduct of the study
Before general anaesthesia patients were routinely assessed for their risk of difficult airway. The variables included inter-incisor distance (IID) measured at maximum mouth opening, thyromental distance (TMD), Mallampati test, head and neck movement (NM), subluxation, body mass, history of difficult intubation and neck circumference (NC). NC was measured at the level of the thyroid cartilage using a cloth tape meter. Furthermore, in the operative time, the drugs used and the Cormack-Lehane (CL) grade were reported on the anaesthesia record. All these data, taken from the different medical records, were signed in a specific case report form. In the case report form, according to the national privacy policy, for each patient only the initials of the first and last name were reported, and a progressive alphanumeric code was assigned to each.
Subsequently, a specific database was prepared in which the data collected were entered. On the basis of the data collected, for each patient, in the initial phase, the El-Ganzouri score (EL.GA) [11] was calculated. The multivariate risk index developed by El-Ganzouri combines and stratifies seven variables derived from parameters and observations individually associated with difficult intubation (Table 1). A final score (obtained by adding the seven variables) > 4 is indicative of difficult intubation. Based on the score, each patient was then classified as NDe (non-difficult expected airways) or De (expected difficult airways). This classification represents the “expected airway” parameter which has been compared with the parameter “real airway”, that is the condition of difficulty (Dr: CL III/IV grades) or non-difficulty (NDr: CL I/II grades) found by the anaesthesiologist at the time of intubation. The intubation manoeuvre was performed by a different experienced anaesthesiologist (10–19 years of experience). A maximum of three intubation attempts, or a maximum of 10 minutes was employed before calling help and moving to an alternative plan. In case of difficult intubation, devices used were the Frova intubating introducer, gum-elastic bougie and the Airtraq. Sensitivity, specificity, and PPV of the EL.GA score relative to our case history were calculated. In the second phase, the median circumference of the neck, according to the body mass index (BMI), of the study sample was chosen as an indicative value of difficult intubation. From this value, the parameter “expected airway” was determined for each patient, then compared with the parameter “real airway”. This analysis was carried out first in the entire sample and subsequently by stratification of the obesity variable.
TABLE 1
el-Ganzouri risk index (EL.GA)
Sample size estimation
A total sample size of 187 (which includes 28 subjects with a CL grade of III/IV) achieves 86% power to detect a change in sensitivity from 0.7 to 0.9 using a one-sided binomial test and 90% power to detect a change in specificity from 0.6 to 0.9 using a two-sided binomial test. The target significance level is 0.05.
Statistical analysis
Univariate analyses were performed to determine clinical factors associated with difficult intubation. Unpaired t-test analysis was used for continuous variables, Pearson’s χ2 test was used for categorical or binary variables, and normality of data distribution was tested using Kolmogorov’s tests. Multiple logistic regression analysis was performed to determine the predictive role of NC, BMI, gender and IID on difficult laryngoscopy measured with the gold standard (CL grade of III/IV). Receiver operating curve (ROC) analysis was performed to determine the NC cut-off as point resulting in the best combination of sensitivity and specificity. All comparisons were conducted at the significance level with the P value less than 0.05. For all cases the sensitivity, specificity and predictive value of EL.GA were calculated and subsequently for the different categories of BMI. For each individual BMI category, the median circumference of the neck was identified. Since the NC could be a surrogate marker of overweight and obesity [19], we decided to identify an NC for each BMI category according the Centers for Disease Control and Prevention (CDC) definitions of adult overweight and obesity [20]. For each BMI category, the median NC was identified; no BMI was less than 18.5, so no patients fell within the underweight range.
RESULTS
In total, 137 women and 103 men (overall, 240 patients) who had an elective surgical procedure, requiring endotracheal intubation, were enrolled. Of these, 48 patients had a CL grade of III/IV (Dr group) and 192 had a CL grade of I/II (NDr group). The patients in the Dr group were significantly older than the patients in the NDr group (P = 0.01): the mean age of the Dr group was 58.19 (SD = 14.05) while the mean age of the NDr group was 48.08 (SD = 16.37).
A significant difference was found regarding height, body mass, BMI and NC between the two groups. The characteristics of the enrolled patients are shown in Table 2.
TABLE 2
Characteristics of enrolled patients
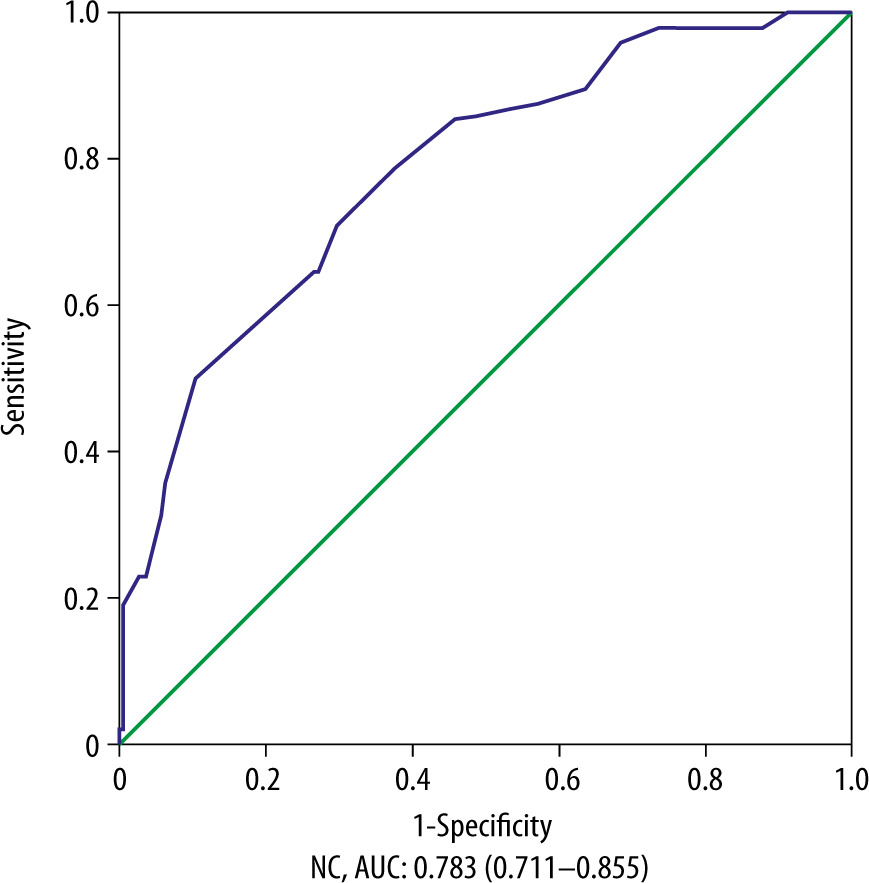
In the multivariable analysis only, NC had a significant association with difficult laryngoscopy (Dr/NDr group): P < 0.001 (Table 3). In patients with class 1 obesity the performance of the EL.GA score was significantly improved (Table 4); the ROC curve analysis determined 42.5 cm as the NC cut-off point resulting in the best combination of sensitivity and specificity, for NC greater than 42.5 cm the likelihood ratio (LR) test decreases in sensitivity with false positive values that remain stable (Figure 1).
TABLE 3
Analysis of explored indicators of difficult laryngoscopy (multiple logistic regression)
| Variables | Odds ratio | 95% CI | Sig. |
|---|---|---|---|
| NC | 1.24 | 1.12–1.37 | 0.00* |
| BMI | 0.98 | 0.91–1.05 | 0.56 |
| Gender | 1.33 | 0.58–3.07 | 0.50 |
| IID | 1.68 | 0.57–4.99 | 0.35 |
TABLE 4
Performance of the EL.GA score and EL.GA+ (EL.GA index adjusted for neck circumference and nutritional status. Nutritional status varies according to body mass index: if BMI is 18.5 to < 25, it falls within the normal; if BMI is 25.0 to < 30, it falls within the overweight; if BMI is 30.0 or higher, it falls within the obese. Obesity is subdivided into 3 categories: Class 1: BMI of 30 to < 35; Class 2: BMI of 35 to < 40; Class 3: BMI of 40 or higher)
| EL.GA score | ||||||
|---|---|---|---|---|---|---|
| Sensitivity | Specificity | PPV | NPV | |||
| Overall | 0.52 (0.37–0.66) | 0.18 (0.09–0.32) | 0.14 (0.06–0.27) | 0.60 (0.45–0.74) | ||
DISCUSSION
The major finding of our study is that EL.GA+, in moderately obese patients, improves the PPV of the EL.GA score, from 0.14 (0.06–0.27) to 0.69 (0.10–0.48). Furthermore, EL.GA+ shows a slightly higher specificity and an identical NPV compared to the EL.GA score.
Our study essentially presents a limit, which is well known, that tracheal intubation is frequently not difficult even when laryngoscopy is difficult, and intubation is frequently difficult even when laryngoscopy is easy. Therefore, prediction methods for difficult laryngoscopy could be not useful. To have an objective, uniform and reproducible criterion we considered a grade 3 and 4 of CL classification system surrogate of difficult intubation; moreover, this criterion is adopted in the literature by a high number of studies on this topic [21–23]. Furthermore, none of the common bedside screening tests is well suited to identify people at high risk of having a difficult laryngoscopy, as many of them are missed [24]. NC measurement is a simple, inexpensive screening measure that can be easily collected during the pre-operative anaesthesiologic visit; therefore, its use was investigated both in association with other scores, as in our study, and as a single variable.
Riad et al. identified an NC above 33.5 cm as an optimal cut-off point for the prediction of difficult intubation in adult women who had to undergo a caesarean section under general anaesthesia; intubation was defined as difficult if the intubation difficulty scale (IDS) was ≥ 5. Sensitivity analysis showed a 100% and 50% specificity with a PPV of 19.2 and NPV of 100 [25]. A larger NC was identified in a study by Paul et al. on a mixed population; the authors identified 34.25 cm as the cut-off value; unfortunately there were missing data on patients’ BMI [26]. Aktas et al. identified as a critical value an NC above 35 cm, in a population with a BMI < of 35; the sensitivity of an NC above 35 cm was 74% with a PPV of 53%. The authors concluded that the combination of NC and sternomental distance, defined as the distance from the suprasternal notch to the mentum (measured with the head fully extended on the neck and the mouth closed), inferior of 13.5 cm was the more accurate predictor of difficult laryngoscopy with a sensitivity of 62% with a PPV of 42% [27]. Highest sensitivity was successively observed by China et al. in a population with a BMI > 35. The sensitivity of an NC above 35 cm was 85.52% with a PPV of 45.76%. The authors found that a combination of Mallampati grade (MPS), SMD, NM and NC permits reliable, accurate and quick preoperative prediction of difficult intubation with a sensitivity of 80% and a specificity of 87% [28]. Rao et al. in a prospective study, designed to evaluate and validate the predictive value of thyromental height test (TMHT) in predicting difficult laryngoscopy, found that an NC above 37.5 had a sensitivity of 65.38%, a specificity of 32.41% with a PPV of 7.98% and an NPV of 91.26%; the BMI of the 340 enrolled patients was 23.4 ± 2.0 [29]. Roh et al. found that the cut-off values for predicting difficult laryngeal exposure (DLE), defined as no part of the vocal folds seen with the anterior commissure laryngoscope, were a BMI > 25.0 and an NC > 39.5 cm. The sensitivity to predict a DLE of an NC above 39.5 cm was 85.52% with a specificity of 71%, a PPV of 32% and an NPV of 89% [30]. The same NC cut-off of 39.5 cm was found by Hirmanpour et al. in a study enrolling adult women who had to undergo a caesarean section under general anaesthesia; the BMI was 30.4 ± 6.7. Analysis showed a 49.06% sensitivity and 89.07% specificity with a PPV of 28.3 and NPV of 95.2 [31]. Kandemir et al. found an NC cut-off of 40.75 cm; in a composite score plus MPS the sensitivity was 43.75%, specificity 66.67%, PPV: 50.00% and NPV: 60.87%; the authors state that the patients in their study were within obesity limits but unfortunately the BMI is not reported [32].
Two studies identified an NC cut-off of 41 cm: in the newest one Han et al. found that an NC cut-off of 41 cm, as a single variable, had a sensitivity 65.7%, specificity 62.9%, PPV 25.8%, NPV: 90.3%; none of the 213 enrolled patients had a BMI higher than 30 [33]. In the oldest one Honarmand et al. found that an NC cut-off of 41 cm, as a single variable, had a sensitivity 26.14%, specificity 98.24%, PPV 71.9, NPV 88.6%; unfortunately in this latest study the authors did not report the BMI, but only a median weight of 68 kg (±11) [34]. An NC closest to that identified by us was found by Gonzalez et al. The authors reported that a difficult intubation, defined as an IDS > 5, was associated with TMD, BMI, MPS and NC; the sensitivity of an NC above 43 cm was 92% with a specificity of 84%, a PPV of 37% and an NPV of 99% [17]. Recently Ozdilek et al. found that NC is not a statistically significant predictor for difficult laryngoscopy in morbidly obese patients [35]. The above-mentioned studies, with their statistical associations, are summarised in Table 5.
TABLE 5
Neck circumference as predictor of difficult airway in adult patients, alone or in association with other variables
[i] NC – neck circumference, BMI – body mass index, p - patient, PPV – positive predictive value, NPV – negative predictive value, MPS – Mallampati grade, SMD – sternomental distance, NM – neck movement, OTI – orotracheal intubation, IDS – Intubation Difficulty Scale, DLE – difficult laryngeal exposure, NA – not available, ULBT – Upper Lip Bite Test
For the several studies presented, it is clear that there is no universally accepted measure as NC cut-off in prediction of poor laryngoscopy; furthermore, the literature data are not even unique in identifying the NC as a predictor of difficult laryngoscopy in morbidly obese patients [35]. Our findings appear to be closest to those reported in the literature by Riad et al.; the authors performed a multiple regression analysis for difficult intubation in morbidly obese patients. They found that a NC > 42 cm and a BMI > 50 kg m−2 were independent predictors of difficult intubation in this patient population [36].
Although a poor laryngoscopy view does not always equate with difficult tracheal intubation, we believe that CL it is the most pragmatic classification for difficult airway management.
Although the CL classification has only been validated in small studies, it is nowadays the gold standard for airway classification both in clinical practice and in airway-related research [37].
The Intubation Difficulty Scale (IDS), a quantitative score that can be used to evaluate intubating conditions [38], could be hypothetically less subjective than CL classification, but at the moment there are no well-conducted studies that directly compare the two classifications.
Another limitation is that in our study the majority of patients are women (137 vs. 103). This is a result of real clinical practice during the enrolment period.
The literature appears to be unambiguous on the fact that difficult intubation is more frequent in obese patients than in non-obese patients [17, 39, 40]. Therefore, the research must be aimed at identifying the best performing predictors of difficult intubation in the obese population, which is growing in most developed countries [41], and is the “testing ground” of the anaesthesiologist.
Although the retrospective nature, small sample size and use of CL classification to identify difficult airways represent important limitations, ours was a pilot study with the aim of obtaining a “proof of concept” on a small sample of the target population, the results of which may be used as “preliminary information” for subsequent, well-designed, prospective studies.
CONCLUSIONS
Based on the results obtained, it is possible to conclude that the EL.GA+ score is a valid composite predictive model to be adopted in the preoperative evaluation phase of the patient, in order to predict difficult airways, in the obese patient. Being a pilot study, based on the first results provided, it should be validated on a larger population with a prospective study. We also believe that in the context of precision medicine, one could evaluate the role of the predictive value of the NC as an additional parameter, through the stratification of other variables.