





The opioid epidemic began with the over-prescription of opioids for palliative care and pain practices, as pain was considered the 5th vital sign by the internal Association for the Study of Pain in 1990 [1]. Overdose deaths have been historically described in three waves, with the first wave starting in the early 1990s with the over-prescription of natural and semisynthetic opioids and methadone [2]. the second wave in 2010 and the third wave in 2013 were due to the overdose of heroin and illicitly manufactured fentanyl [3–6]. More recently, there have been increased reports of the use of illicitly manufactured fentanyl, fentanyl-related substances, and other opioid-related substances (i.e., U-47700) either alone or in combination with heroin [7–14].
The opioid epidemic contributes to the deaths related to opioid overdose or misuse and weakens a country’s economy. According to a systematic review including six studies with 810 patients who underwent different surgical procedures, postoperative opioids often remain unused and undisposed [15]. this overprescribed, unused drug is considered a source for the dispersion of opioids in the community and is a new contributing factor to the current opioid epidemic [16].
THE OPIOID EPIDEMIC IN THE INTENSIVE CARE UNIT
Intensive care units (ICUs) have witnessed a rise in opioid-related overdoses, with admissions for overdoses increasing by 34% between 2009 and 2015. Furthermore, the mortality rate of critically ill patients hospitalised for overdose rose from 7.3% to 9.8% during the same period [17]. there is undoubtedly a need for critical care practitioners to be aware of opioid use disorders since there are an increasing number of patients who receive opioids in the ICU environment. in one study, almost 80% of patients on mechanical ventilation were administered opioids, and this figure increased to over 90% for patients on mechanical ventilation for more than seven days [18]. Additionally, these hospitalisations might result in increased hospital and societal expenses since this group may need an increasing amount of sophisticated and costly multi-organ support. Stevens et al. [17] estimated a nearly 60% increase in the cost of each opioid overdose ICU hospitalisation, demonstrating the strain on the healthcare system caused by the opioid crisis.
Different reports have shown a sharp rise in morbidity and mortality from opioid overdose and misuse during the coronavirus disease 2019 (COVID-19) pandemic [19]. A recent report has shown that the number of cases of opioid overdoses increased in Kentucky during the early weeks of the COVID-19 pandemic [20]. Deaths due to synthetic opioids increased 38.4% in the 12 months ending in June 2019 compared with the 12 months ending in May 2020, which made the opioid epidemic worsen [21]. there was a 35% increase in test positivity for non-prescribed fentanyl and a 44% increase for heroin during the COVID-19 pandemic [22]. the sharp rise in medical issues related to opioid misuse is related to the unavailability of opioids for chronic pain management, financial insecurity, and loss of jobs [23]. Restrictive opioid-prescribing early in the COVID-19 pandemic can lead to reflex over-prescribing later to avoid frequent wasteful visits for refills, and reflex over-prescribing also occurs due to an over-correction for earlier under-prescribing [24]. in the early COVID-19 pandemic, the availability of opioids was slightly hampered among the patients dependent on opioid analgesics, but later, clinicians adjusted the prescription to include larger quantities [25]. while COVID-19 imposed several significant barriers to treatment for these people, it was also accompanied by changes that improved access to care. these measures include lowering financial obstacles to treatment via an emergency Medicaid expansion and increasing the use of telemedicine in the care of people with opioid use disorder [26]. the guidance released by the Substance Abuse and Mental Health Services Administration (SAMHSA) during the COVID-19 pandemic had a potential risk of non-medical use of methadone in a patient with an opioid use disorder [27]. to address this issue, patients receiving take-home methadone should be co-prescribed naloxone, which may lower the risk of lethal overdose.
Patients with COVID-19 pneumonia and a preexisting opioid abuse disorder have increased mortality and morbidity. Patients with opioid use disorder have increased odds of hospitalisation, length of stay, and invasive ventilation requirements due to COVID-19 [28]. the cDc recommended expanding naloxone distribution, awareness about substance use disorders, early detection, and intervention to combat the crisis [29].
India is sandwiched between major opium- producing countries such as Afghanistan, Myanmar, and thailand. Apart from that, india is becoming a central production hub for opium for the legal pharmaceutical market. Synthetic opioids have been out of reach for the general population due to restrictions placed by the government of india [30–32]. india has the second-highest population globally, but the irony is that less than 1% of people receive pain management and palliative care services [33]. Many patients suffering from chronic pain due to cancer are out of reach of adequate opioid analgesics.
In contrast, there is a parallel increase in the prevalence of heroin addiction in some parts of india [34]. According to different survey reports, it is clear that drug abuse in india has increased [35, 36]. india’s three major poppy-growing states are Rajasthan, Madhya Pradesh, and Rajasthan. According to an observational study conducted in 45 rural villages of Rajasthan province of india’s Barmer, Jaisalmer, and Bikaner districts, the addiction rate was 8.4%, 79%, and 6.9%, respectively [37]. Malviya et al. [38] conducted a prospective cohort study from December 2004 to February 2006 in a tertiary hospital in western Rajasthan; they found a higher incidence of postoperative respiratory, cardiovascular, systemic, and local complications associated with patients with opioid use disorders.
Although not labelled as an opioid epidemic like in the United States, there is a possibility of a significant impact of opioid use on general health due to an amendment to the Narcotic Drugs and Psychotropic Substances (NDPS) Act in 2014 [39]. this law prevents illicit opioids while promoting the medical and scientific use of essential opioids. Due to the need for multiple licenses, state permissions, and complexities, opioids are less accessible for general use, exacerbating the opioid crisis. in many states of india, there is an increased report of drug trafficking and opioid-associated medical issues among young adults [40–43]. Opium use has been integrated into social customs in some parts of the country and has become a social, mental, and economic burden [44, 45]. this opioid use disorder led to hospitalisation for intoxication and issues related to opioid withdrawal [46].
OPIOID ADDICTION DISORDERS
According to DSM-5, the criteria for opioid use disorder include the presence of at least 2 out of the following 11 criteria [47]:
consumption of opioids in larger amounts and for a longer period;
persistent desire to control opioid use, the strong desire to take opioid;
much more time is spent to obtain opioids, use them and recover from their effects;
strong urge to use opioids;
failure to complete major role obligations at the workplace;
continued opioid use despite persistent social issues caused by the effects of opioids;
reduced social, occupational, and recreational activities;
recurrent opioid use in a physically hazardous situation;
continued opioid use despite knowing its recurrent physical and psychological hazards;
opioid tolerance;
withdrawal symptoms.
The severity of opioid use disorder can be graded based on the number of symptoms/criteria present (mild = 2–3, moderate = 4–5, severe = 6 or more).
A patient with an opioid use disorder can present in various forms in the ICU. these can include the following types of problems and complications faced by intensivists during patient management:
acute, life-threatening intoxication;
the opioid-addicted patient presents with a critical illness;
opioid withdrawal (including iatrogenic) in the critical care setting;
perioperative management of patients with opioid addiction or chronic opioid use for medical purposes;
pain management for acute or chronic illnesses;
complications due to chronic opioid use are similar to those from other drug abuse, such as the risk of Hiv and other infections and skin infections;
chronic intensive care related to pain.
Managing a patient with an opioid use disorder can be extremely difficult for a health care provider. the challenge for an intensivist starts with the patient with an acute life-threatening overdose of opioids in an emergency and lasts until discharge and rehabilitation therapy. According to one study, opioid overdose is associated with simultaneous consumption of other agents such as alcohol, marijuana, lysergic acid diethylamide (LSD), amphe tamine, benzodiazepines, and cocaine [48]. concurrent use of various illicit substances further complicates the management of these patients.
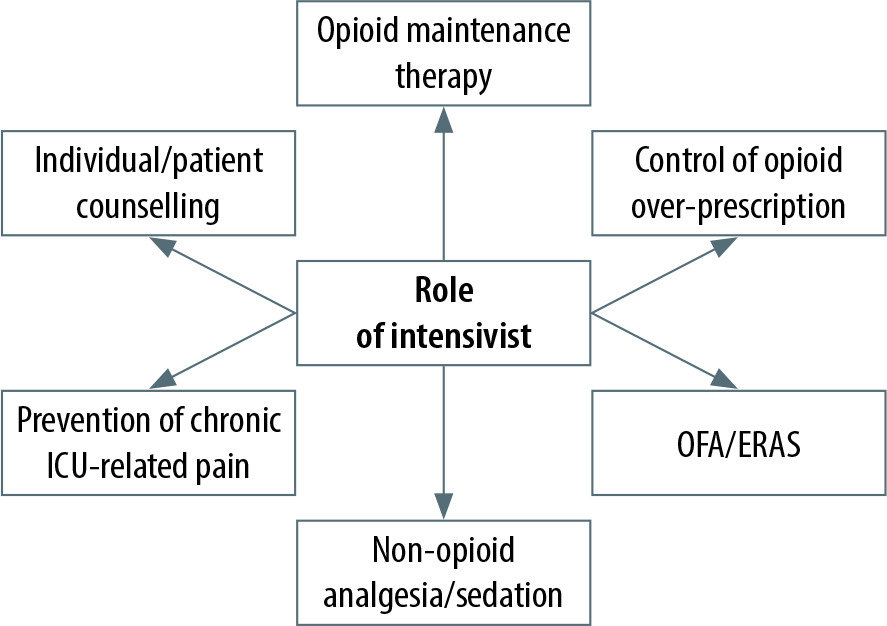
THE ROLE OF THE INTENSIVIST IN COMBATING THE OPIOID EPIDEMIC
According to a recent report from the world Health Organization (WHO), 0.5 million deaths are due to drug abuse, with 70% involving opioids and 30% of deaths due to overdose [49]. Opioid-related deaths in 2019 quadrupled compared to 1999 [50]. the COVID-19 pandemic has accelerated the rate of death associated with synthetic opioids in the USA [51]. the United States Department of Health and Human Services initiated a 5-point strategy to combat the opioid epidemic, including better addiction prevention and recovery services, data collection, research, pain management, and the availability of overdose-reversing drugs [52].
Pain is considered the fifth vital sign, and adequate analgesia in ICU patients is one of the prime areas of concern. Acute pain is often undertreated in opioid-dependent patients admitted to the intensive care unit. Postsurgical pain, immobility, indwelling devices, and procedures during an ICU stay such as chest tube removal, wound drain removal, and arterial line insertion can contribute to acute pain in these patients [53]. Failure to manage acute pain can lead to agitation, sympathetic overactivity, neurobehavioral changes, and progression to chronic pain in ICU patients [54]. Opioids are the mainstay treatment for acute pain in the ICU. Patients with opioid addiction should maintain their pre-existing opioid agonist treatment, supplemented with short-acting analgesics as required for acute pain. when prescribing opioids to patients, the intensivist should be cautious regarding the history of opioid addiction as well as the potential risk of opioid tolerance, dependence, and addiction among ICU survivors (Figure 1). Among ICU survivors, opioid prescribing is higher in postsurgical patients than in medical patients [55].
One of the adverse effects of chronic pain therapy is opioid misuse, hampering immunity and sometimes resulting in overdose. chronic opioid treatment impairs macrophage progenitor cells and lymphocyte proliferation. Furthermore, opioids have a considerable effect on the differentiated activities of immune cells. Opioids accomplish this by acting directly on target cells or indirectly through centrally mediated pathways [56].
Various medications including methadone, buprenorphine, naltrexone, buprenorphine with naltrexone combination, and levomethadyl acetate/levo-alpha-acetylmethadol are used and well studied for opioid use disorder as maintenance or detoxification therapy (Table 1). Buprenorphine, methadone, and naltrexone are the drugs used for medication-assisted treatment. According to the national practice guideline by the American Society of Addiction Medicine, psychosocial therapy should be offered to patients on oral therapy and extended-release naltrexone [57]. the role of an extended-release formulation of naltrexone without psychosocial therapy has not been established. Out of the above three drugs, buprenorphine and methadone are categorized as essential drugs according toby the WHO [58].
TABLE 1
Various medications used for opioid use disorder substance
| Substance | Mechanism of action |
|---|---|
| Methadone, LAAM | Opioid agonist |
| Buprenorphine | Opioid partial agonist |
| Naltrexone | Opioid antagonist |
| Buprenorphine/– naltrexone | Opioid partial agonist/antagonist |
| Lofexidine | α2 agonist |
Methadone is an FDA-approved drug for opioid detoxication and maintenance therapy. it is a muopioid receptor agonist and has properties similar to morphine. l-methadone has 5–30 times higher potency than D-methadone, lacking addiction potential and respiratory depressant effects. Properties such as adequate oral bioavailability, longer duration of action, and an extended duration of withdrawal suppressing effects in the opioid-addicted patient make methadone maintenance therapy attractive to physicians. Other impacts on cough suppression, action on biliary tone, and other effects are similar to morphine. Plasma levels are detectable 30 minutes following oral ingestion and peak at 4 hours. the liver is the primary organ of metabolism, and pyrrolidine and pyrroline are the primary metabolites. the half-life of methadone is 15–40 hours. there is a risk of drug accumulation after repeated administration. the respiratory depressant effects lag behind the peak analgesia. tolerance and dependence are not uncommon with methadone, as with other opiates. the typical dose used for maintenance therapy is 2.5 to 10 mg every 8 to 12 hours. the adverse effects of methadone are similar to those of other opiates. in addition to the typical side effects, the adverse effect that needs partICUlar attention is Qt prolongation. close cardiac monitoring must be done, especially when the patient is on multiple drugs causing Qt prolongation [59]. A retrospective study conducted by Patel et al. [60] from 2012 to 2016 in the ICU found no significant increase in Qtc interval with low-dose methadone therapy. in critically ill patients, protocolised methadone therapy reduces the length of mechanical ventilation, weans from opiate infusion, and improves the prognosis [61].
Buprenorphine, a mu receptor partial agonist, kappa antagonist, delta agonist, and ORl-1 receptor partial agonist, is commonly used for opioid use disorder as maintenance therapy. the peculiar pharmacological profile (only a ceiling effect on respiratory depression, not analgesic properties) attracts physicians to use buprenorphine in an office-based setting, unlike methadone, which is mainly prescribed in authorized deaddiction centres [62]. Buprenorphine has less toxicity due to overdose. Different formulations of buprenorphine are used and studied for maintenance therapy and chronic pain [63, 64]. Buprenorphine buccal film has been studied for chronic low back pain [65]. the sublingual route is preferred for opioid maintenance therapy.
Buprenorphine rotation is a promising new strategy that can be used instead of tapering long-term opioid therapy (ltOt). A systematic review conducted by Powell et al. [66], including 22 studies, showed that buprenorphine therapy reduced chronic pain intensity without precipitating opioid withdrawal symptoms. A novel strategy for starting buprenorphine and naloxone has been described in a critically ill intubated patient with an opioid use disorder using a rapid micro-induction (micro- dosing) technique. it entails the use of small, frequent doses of buprenorphine or naloxone that do not trigger withdrawal symptoms [67]. According to the results of a prospective study, it was found that the use of buprenorphine and naloxone improved sleep and depression when used for medication-assisted therapy [68]. According to the recommendation of Nice guidelines in the UK, buprenorphine and methadone are the first-line therapies for both opioid maintenance and medically assisted withdrawal therapy [69]. in opioid substitution therapy, buprenorphine is six times safer than methadone in the event of a drug overdose [70]. in the SUMMit trial involving 361 opiate-dependent individuals, patients on methadone therapy had higher incidence of substance abuse and physical and psychiatric issues than those on buprenorphine [71]. Due to the abuse potential and severe adverse effects of a methadone drug overdose, such as respiratory depression and Qt prolongation, the naloxone-buprenorphine combination has gained importance. this drug combination has less abuse potential. Buprenorphine and naloxone are available in a 4 : 1 ratio.
The FDA approved levo-methyl acetate hydro-chloride (lAAM) for maintenance therapy in 1993 [72]. According to a review, lAAM therapy is associated with less use of heroin, but adherence to therapy is better than methadone therapy [73]. However, owing to the Qt prolongation and torsade de pointes effects due to the potassium channel blocking effects [74], the european Medical Agency suspended the marketing of lAAM in 2001. the United States Food and Drug Administration placed a black box warning on the label for lAAM [75]. induction with a higher dose of lAAM may be associated with a higher patient dropout rate as well as an adverse effect [76].
Opioid antagonists such as naltrexone block the euphoric effect of opiates and prevent physical dependence due to opioid addiction. intramuscular extended-release naltrexone is approved by the Food and Drug Administration for treating opioid and alcohol use disorders [77]. Due to the poor adherence risk with oral naltrexone therapy, sustained-release naltrexone preparations have been developed. Naltrexone therapy with either individual or group psychosocial therapy is associated with a better outcome [78]. tramadol may be considered an alternative to methadone or buprenorphine for opioid withdrawal symptoms, but studies are limited [79].
NON-OPIOID THERAPY IN THE INTENSIVE CARE UNIT
Opioids are the primary pharmacological agent for analgo-sedation in the intensive care unit. Given concerns regarding the opioid epidemic, non- opioid analgesic agents should be used to combat the crisis. According to one recent systematic review and meta-analysis, the use of adjuvant anal-gesic agents in addition to an opioid was associated with a reduced pain score at 24 h as compared to opioid alone therapy [79]. Opioid consumption was reduced using adjuvant analgesic agents (in oral morphine equivalents per 24 h, 25.89 mg less; 95% ci: 19.97–31.81 mg) [80].
According to the PADiS algorithm, individuals at risk of opioid-related adverse effects should receive an adjuvant non-opioid-based analgesic [81]. Nociceptive pain can be managed with acetaminophen, nefopam, or low-dose ketamine, whereas neuropathic pain can be managed with gabapentin, pregabalin, and carbamazepine.
In the ICU, non-opioid analgesics and adjuvant agents such as neuropathic agents are alternatives to opioid use in these patients.
According to one study, 64% of patients receive paracetamol in the ICU [82]. it is a safe and effective option for ICU patients. Paracetamol is available in intravenous, oral, and rectal preparations [83].
Non-steroidal anti-inflammatory drugs (NSAiDs) block the cOX-1 and cOX-2 receptors and decrease prostaglandin synthesis. Apart from postoperative patients admitted to the ICU, there are limited data regarding the analgesic efficacy of NSAiDs in critically ill patients [84]. NSAiDs should be avoided in patients with allergies, renal dysfunction, gastrointestinal bleeding, and platelet dysfunction. Because of these predicted adverse effects, PADiS guidelines advise against the routine use of NSAiDs despite their opioid-sparing effects [81].
Ketamine is an analgesic and sedative agent that acts as an NMDA receptor antagonist. low-dose ketamine infusion in ICU patients is associated with reduced opioid requirements and a minimal impact on haemodynamics [85].
Other non-opioid drugs are worth considering, for example, a-2 agonists, whose central sympatholytic effects are potentially useful in managing opioid withdrawal symptoms. clonidine was popularised as a non-opioid agent for relieving withdrawal symptoms [86], but hypotension is a significant side effect of clonidine that limits its use. lofexidine is one of the drugs in that group studied to treat opioidwithdrawal disorder [87]. Medication-assisted the rapy (MAT) is a combination of medications with behavio ural or psychosocial counselling for opioid addicts [88]. Psychosocial treatment has a better outcome profile than treatments with only medications [89]. MAT has a role in decreasing opioid-related deaths, infectious disease transmission, and criminal activities resulting from opioid dependence [88]. the goal of psychosocial therapy should include assessing psychosocial needs, supportive counselling, behaviour therapy to adhere to the prescribed medication, individual, group, or family counselling, and treatment of other psychiatric disorders [89, 90]. counselling the patient and caregiver is crucial in rehabilitation programmes and prevents post-intensive care opioid dependence. One should be aware of the potential risks associated with opioid analgesics, including the risk of dependence, tolerance, and danger signs of overdose. Acupuncture, transcutaneous electrical nerve stimulation (teNS), massage, and music therapy may be beneficial adjuncts to drugs in these individuals’ pain management. in opioid-dependent individuals, regional analgesia may be an effective adjunct to systemic analgesics [91].
OPIOID WITHDRAWAL
Due to the increased importance of analgosedation in the ICU to prevent the risk of delirium, opioids have become a vital agent for analgesia. According to one study, the overall incidence of iatrogenic opioid withdrawal was 16.7% and it was associated with continuous opioid infusion for more than three days [92]. iatrogenic opioid withdrawal is mainly observed with remifentanil, fentanyl, and morphine [93]. there are many strategies to treat this opioid withdrawal in ICU patients, e.g. substituting short-acting opioids with longer-acting opioids and gradually decreasing opioids in a stepwise manner [91]. the intensivist’s role is to prevent episodes of iatrogenic opioid withdrawal by adapting non-opioid-based analgesic agents and using regional analgesia [94].
These patients may develop opioid withdrawal symptoms, and methadone, buprenorphine, cloni-dine, and lofexidine are generally prescribed to combat this issue. the selective a-2 agonist dexmedetomidine has been administered to treat the hyperactive symptoms of opiate withdrawal [91]. Adequate titration of opioids for appropriate anal-gesia in a patient with withdrawal is a challenge for intensivists, and there is no definite guideline regarding the issue. the clinical Opioid withdrawal Scale (cOwS) is a valuable tool for deciding the need and dose of a pharmacologic agent for opioid withdrawal [95]. Sometimes, in patients with a history of addiction to crude opium preparations, it is difficult to determine the actual dose and composition of opioids. compliance with pharmacologic therapy is not always adequate, which leads to the discontinuation of therapy and switching to crude preparations [96]. counselling of the caregiver regarding the need for maintenance and drug therapy is an essential component.
CHRONIC ICU-RELATED PAIN
Another major issue that should not be overlooked is persistent pain in ICU survivors. Diffe rent researchers have a wide range of definitions of persistent or chronic ICU-related pain (CIRP) [97]. the highest incidence rates of persistent pain are 77% and 36% after three months and two years after ICU discharge [98]. the adverse consequences of CIRP lead to prolonged opioid use in intensive care survivors and the progression to opioid addiction. Duration and intensity of pain are the risk factors for developing CIRP. A multimodal analgesic approach with non-opioid analgesics should be used to prevent CIRP.
Postoperative pain has multiple complications, including cardiovascular effects due to activation of the sympathetic nervous system, risk of thromboembolism and progression to chronic pain, and increased hospital stay. Opioids have been the primary pharmacological medicine for perioperative analgesia. However, opioid use in the perioperative period could promote the long-term use of opioids. chronic opioid dependence is associated with risk factors such as pre-operative tobacco or alcohol abuse, younger age group, mood disorders, and pain disorders. the American college of Surgeons and the American Society of Anesthesiologists suggested non-opioid analgesic agents for perioperative pain control and calculated the use of opioids on discharge prescriptions [99]. Multimodal analgesia with non-opioid analgesic agents, anti-depressants, and anticonvulsants are some promising options for preventing opioid-related adverse effects in the ICU.
CONCLUSIONS
The opioid epidemic is a real threat to the nation’s health and from a socio-economical point of view. control and monitoring of over-prescription of opioids should be carried out to combat the opioid epidemic. Preference for non-opioid analgesics, management of acute pain in the ICU to prevent chronic pain syndromes, and education of patients and their care providers are vital to preventing this epidemic. the opioid-sparing strategy should be followed in the early postoperative period in the intensive care unit. Maintenance therapy with either methadone or buprenorphine and psychosocial counselling of the individual and their family members are vital to treat opioid addiction. An inten sivist should plan opioid detoxification or maintenance therapy after the clinical improvement of ICU patients.