
Patients with end-stage renal disease (ESRD) are at increased risk of haemostasis disorders which result from changes in plasma and platelet (PLT) components [1]. Haemodialysis (HD) is the most common method of treatment used in patients with ESRD [2]. The contact between blood and the artificial surfaces of dialysis machines increases PLT reactivity and the production of coagulation factors. Consequently, this may lead to the occurrence of coagulopathy. It may also affect the natural process of blood clot dissolution (fibrinolysis) [3]. Concomitantly, damage in the vascular endothelium and changes in the activity of proteins participating in the coagulation cascade during the course of the ESRD may pose a risk of haemorrhage [1]. Furthermore, HD may only replace about 10% of proper kidney function, thus it does not allow for total elimination of chronically increased urea and does not prevent it from impacting on the coagulation system [4].
The formation of stable blood clots, which are composed of fibrin fibres and PLTs, is a core stage of haemostasis. This is possible because of the formation of fibrinogen receptor GPIIb/IIIa complex on the PLT surface. If disturbed, it leads to severe haemorrhagic diatheses, including Glanzmann’s thrombasthenia (inherited disorder of GPIIb/IIIa receptor) or afibrinogenemia [5, 6].
Platelet levels and fibrinogen concentrations are measured using standard laboratory tests, however, normal PLT function and fibrinogen polymerisation are equally important [6, 7].
Global haemostasis assays (GHA) are required for this assessment. Currently, technological advances allow for bedside testing (point-of-care tests – POCTs) that have dramatically decreased the diagnosis time [8]. Compared to standard coagulation tests, the GHA-POCTs introduces a new level of quality in the assessment of haemostasis potential of the whole blood [9].
Recently, the development and propagation of GHA-POCTs has been observed. This is a diagnostic method which allows for the assessment of dynamics of the whole blood clot formation and its quality, including a unique possibility to assess fibrinogen polymerisation and the course of the fibrinolysis process [10], whereas multiple electrode aggregometry (MEA) is used to monitor the processes of PLT adhesion and aggregation.
The European guidelines on the management of major bleeding recommends the abovementioned GHA-POCT as an effective diagnostic method for assessing haemostasis [11, 12].
This study aims to determine the haemostatic profile in a group of patients with ESRD on chronic, interrupted dialysis, especially in terms of PLT function and the impact of in vitro fibrinogen supplementation on clot properties.
METHODS
Study design
This prospective study with a control group was approved by the Bioethics Committee of the Medical University of Warsaw (KB/244/2013). Informed written consent was obtained from all participants.
The number of patients was determined using the assumption that there is a 30% difference in GHA-POCT parameters to confirm their significance (α = 0.05, β = 0.8). Initially, a total of 47 adult patients were recruited.
The study group (haemodialysis group – HD group) comprised 23 patients on chronic dialysis (three times a week for more than 2 years). Congenital or drug-induced haemostasis disorders (excluding the use of 75 mg per day of acetylsalicylic acid) were set as exclusion criteria. A total of 24 persons with no history of renal diseases or coagulopathy were enrolled to the control group (healthy control group – HC group).
The data for 44 patients were finally analysed, with 22 persons in each group. Two patients were excluded from the analysis because of the unacceptably prolonged time of the pre-analytical phase of the blood sample (the analysis could not be started within 120 minutes of taking the blood sample). One patient was removed because of their baseline PLT level; i.e. PLT < 100 G L-1. This is considered to be a methodological limitation of the MEA. All study participants were fully acquainted with the study protocol and their written consent to participate in this study.
Diagnostics of coagulation system
Thromboelastometry was performed using ROTEM Delta (Tem Innovation GmbH, Munich, Germany). Platelet function using MEA was assessed by Multiplate (Roche, Basel, Switzerland). Standard laboratory testing of the coagulation system was performed, and complete blood counts were obtained for all study participants.
In the study group, blood was collected from arteriovenous fistula prior to the HD and the application of low molecular weight heparin. A nearly two-day period between the last HD and blood collection guaranteed the presence of severe haemostasis disorders resulting from the effects of urea and other metabolic products on the coagulation.
In the HC group, blood was collected by one-time puncturing of the basilic vein. A vascular tourniquet was not applied in order to avoid the disorders of blood flow and activation of the coagulation system.
A total of 20 mL blood was collected from each study participant. Sodium citrate vacuum tubes (using ROTEM) and hirudin tubes (using Multiplate) were used. Testing was performed in accordance with the manufacturer’s instructions [13, 14].
EXTEM and FIBTEM screening were applied. EXTEM provides information on the extrinsic pathway of coagulation. The addition of cytochalasin D, as an inhibitor of PLT with FIBTEM, shows the picture of a fibrinogen clot that is formed without the contribution of PLT, which is dependent on the quality of fibrinogen polymerisation [6]. EXTEM was also used to analyse the clot lysis. All tests were performed for at least one hour. Assessed parameters included clotting time (CT), maximum clot firmness (MCF), and maximum lysis (ML) [15].
The MEA TRAPtest was applied to determine the PLT aggregation, which is dependent on the GPIIb/IIIa receptor. TRAPtest is considered to be the most reliable method to assess the aggregation potential of thrombocytes [16]. The majority of patients (15/22) from the study group simultaneously took ASA; thus, an ASPItest was conducted. This test is used to monitor the effectiveness of the PLT aggregation blockade that is dependent on the activation of arachidonic acid. The aggregation registered by MEA is presented as the area under the curve (AUC, [AU*min]). A cut-off value of 300 AU*min for an effective ASA-induced PLT blockade was determined [17].
In vitro fibrinogen supplementation
Normal fibrinogen concentration does not prevent polymerisation disorders. Toxins, which are the end-products of protein catabolism in patients with ESRD, lead to qualitative disorders of fibrinogen. Increased carbamylation (a non-enzymatic, irreversible protein modification) is one of the negative processes associated with uraemia, which considerably affects the spatial structure of fibrinogen polymerisation [18].
In HD and HC groups, the fibrinogen concentration in peripheral blood was measured using the Clauss method, which is based on the thrombin clotting time. This is one of the most common methods used in clinical practice [19]. EXTEM, FIBTEM, and TRAPtest were repeated for all blood samples with 80 µL of in vitro fibrinogen concentrate (FIBR) (Haemocomplettan, CSL Behring, King of Prussia, PA, USA). The results were compared with the baseline values (before FIBR) to determine its impact on clot formation and PLT aggregation. The in vitro dose of FIBR corresponded to the intravenous dose of 4 γ in a patient weighing 70 kg. It was determined on the basis of earlier literature reports [20].
Statistical analysis
Statistical analysis was carried out using Statistica 13 (TIBCO Software, Palo Alto, CA, USA). A Kolmogorov-Smirnov test was applied to analyse the data for normality distribution. Based on the distribution properties, the data was described using the mean (±SD) or median (Q1–Q3). A one-way analysis of variance (the Mann-Whitney U test) was used to show the differences in non-parametric tests. An analogical analysis of the data of parametric distribution was carried out using Student’s t-test. The analysis of differences for repeated measures was used for dependent variables (haemostasis parameters before and after fibrinogen supplementation). Statistical significance was determined to be P < 0.05.
RESULTS
Characteristics of the groups and baseline results of standard laboratory testing
This study was conducted from November 2013 to August 2016. Table 1 presents the characteristics of each group, including baseline parameters and laboratory testing results.
TABLE 1
Demographic and clinical characteristics of the groups
[i] Data are presented as mean ±standard deviation or median (25th–75th percentile) based on the distribution properties
The analysed groups differed in terms of age. No differences in the number of PLTs and the clotting time via the intrinsic and extrinsic pathways were observed between the groups. In the HD group, the prolongation of thrombin time, which describes the common pathway of clotting time, was statistically significant but was within the range of reference values.
Baseline results of global haemostasis assays
Thromboelastometry showed a significant prolongation of CT in the EXTEM assay in the HD group compared to the HC group. MCF EXTEM did not differ significantly between the groups. Contrary to this, MCF FIBTEM was significantly higher in the HD group (Table 2). In the EXTEM assay, hyperfibrinolysis (ML > 15%) up to 60 minutes was not observed in all participants.
TABLE 2
Characteristics of global haemostasis assay and point-of-care test (GHA-POCT) describing the whole blood clot formation and platelet aggregation in both groups
The activation of the GPIIb/IIIa-fibrinogen complex, which was assessed using TRAPtest, showed significantly impaired aggregation in the HD group (Table 2).
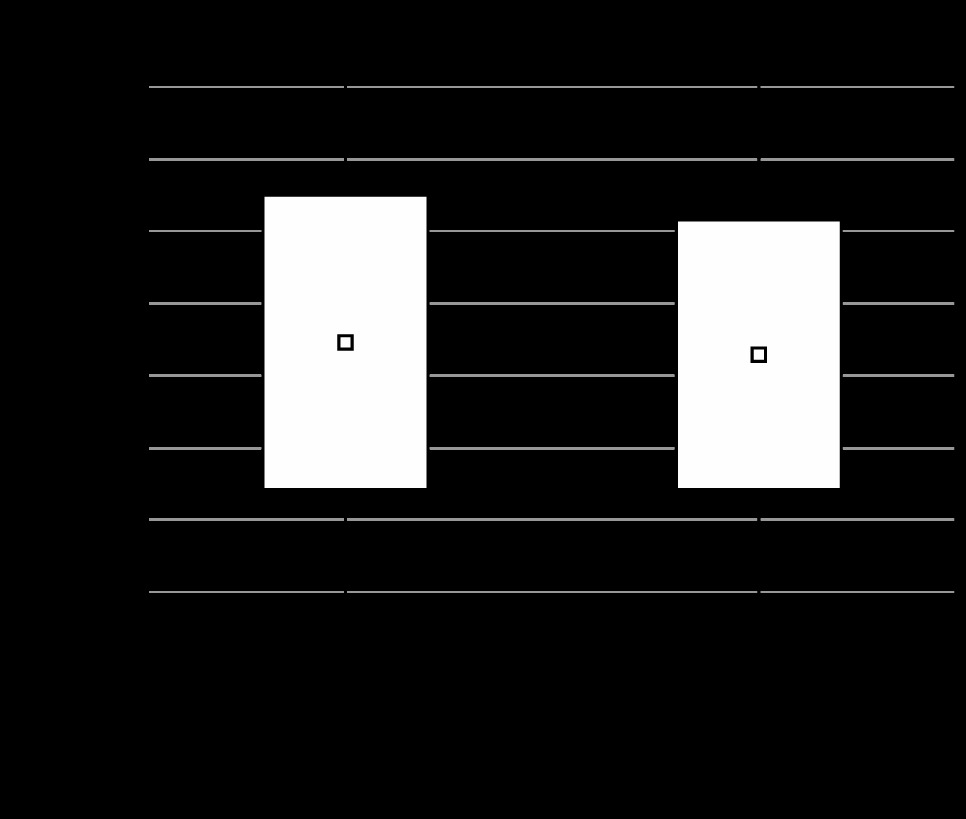
The ASPItest revealed significantly lower PLT activation in all patients from the HD group with chronic ASA intake (15/22, 68%) compared to the dialyzed patients who did not take ASA and the control group. The TRAPtest did not show significant differences between the patients on dialysis from ASA and non-ASA groups (Figure 1).
Effects of fibrinogen concentrate supplementation on the results of global haemostasis assays
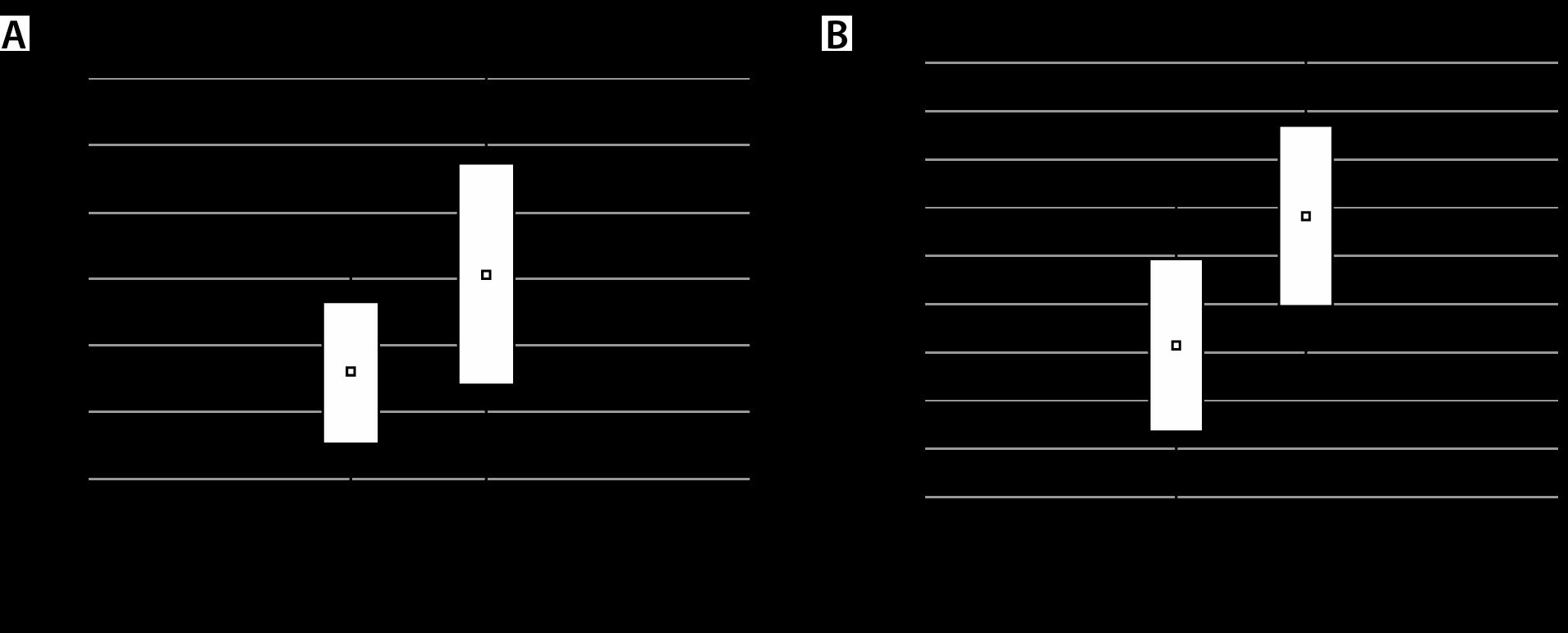
FIBTEM revealed a statistically significant improvement of MCF following the supplementation of fibrinogen concentrate in both groups (P < 0.001) (Figure 2).
FIGURE 2
A) Effects of fibrinogen concentrate supplementation on the MCF in FIBTEM in HD group. B) Effects of fibrinogen concentrate supplementation on the MCF in FIBTEM in HC group
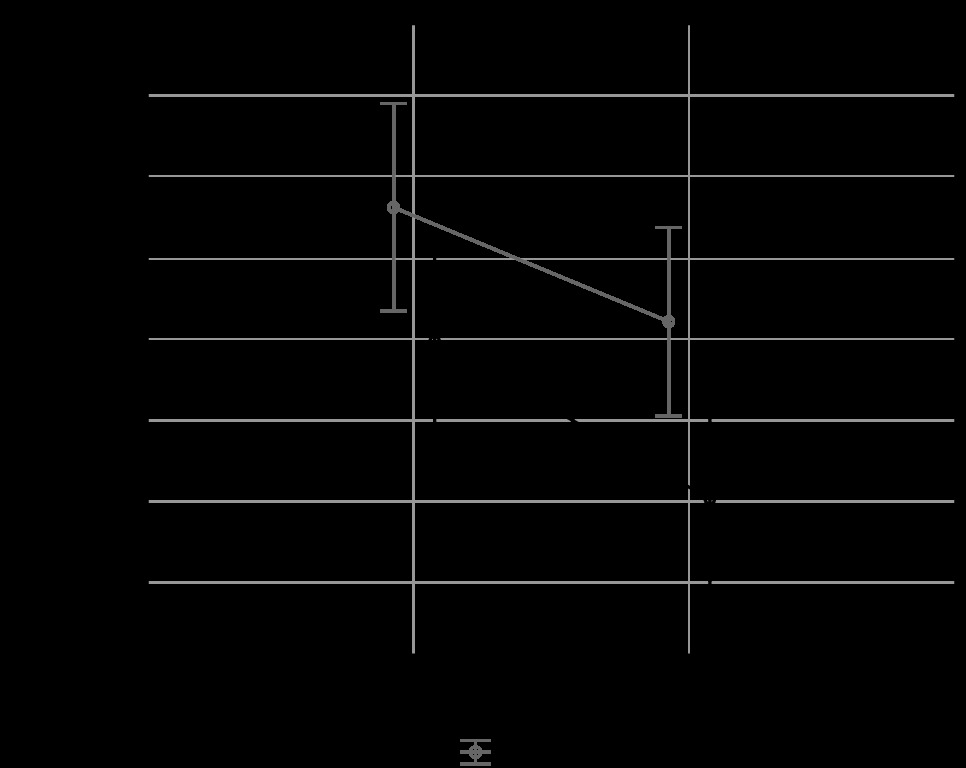
The TRAPtest showed no improvement in the PLT aggregation following the in vitro fibrinogen concentrate supplementation (Figure 3). No positive effect was reported in both groups. Furthermore, it was observed that the results of the TRAPtest after the administration of fibrinogen were lower compared to the baseline values; however, this difference was not considered statistically significant.
DISCUSSION
Our study confirmed the presence of complex and multifactorial coagulation disorders in a group of patients with ESRD on chronic HD. The results of GHA-POCT were often conflicting. Prolonged CT EXTEM, which is associated with the activity of coagulation factors (II, V, VII, X) and PLT, may be responsible for the enhanced susceptibility to haemorrhages. Increased risk of thromboembolic complications may result from the higher activity of fibrinogen component of the clot (MCF FIBTEM) compared to the HC group. A possible cause of this condition may be chronic inflammation in ESRD patients [21].
The effects of uraemia on the function of PLT is common knowledge [22]. The mechanism of this correlation is a complex issue. Lutz et al. state that it results from the abnormal binding of fibrinogen with activated PLT [23]. It is suggested that it is associated with the action of uremic toxins which impair the functioning of GPIIb/IIIa receptor complex [4] irrespective of the fact that the former analysis of urea concentration as a marker of uremic toxins conducted by Remuzzi et al. did not reveal its correlation with the time of bleeding [24].
In our study, the number of PLTs in both groups was normal (Table 1). However, a considerable impairment of thrombocyte function was reported in the HD group (decreased aggregation in TRAPtest). The limited activity of the GPIIb/IIIa-fibrinogen complex in this group was in accordance with earlier literature reports [25, 26] and the results of the GHA-POCT [27, 28].
Impaired PLT aggregation may be explained by the study carried out by Moal et al. [29]. They suggest that there is lower expression of surface antigens of GPIIb/IIIa receptor after stimulation with thrombin receptor-activating peptide-6 (TRAP-6) in patients with the ESRD on HD compared to the control group. The expression of GPIIb/IIIa was indirectly determined through the number of binding site antibodies per PLT (BSAP).
The ASPItest confirmed the effectiveness of MEA in the assessment of the blockade of the PLT activation pathway. Simultaneously, it was shown that ASA does not affect the TRAP-6-induced aggregation. This is in accordance with the earlier reports by Jambor et al., who suggest that the effect of aggregation in this pathway is unresponsive to cyclooxygenase type 1 (COX-1) inhibitors [17].
Fibrinogen supplementation is a well-known method for substitution therapy of coagulopathy. In spite of a higher baseline concentration of fibrinogen in the HD group compared to the HC group, the legitimacy of its supplementation was based on impaired fibrinogen function. Having considered all the above, the authors expected that qualitative fibrinogen disorder would be compensated through the addition of high-quality fibrinogen concentrate.
Fibrinogen supplementation resulted in the improvement of MCF as measured by FIBTEM, which confirms the effectiveness of the in vitro method that was used. Furthermore, this agrees with other studies which confirmed a strong correlation between fibrinogen polymerisation and MCF FIBTEM value [30, 31].
A hypothesis about the possible improvement of PLT aggregation after fibrinogen supplementation was based on the earlier reports suggesting its positive effect on PLT aggregation in a group of patients taking GPIIb/IIIa inhibitors [32].
Lang et al. showed that an improvement in clot properties was achieved by the increase in fibrinogen concentration in a group of patients with coagulation disorders associated with severe thrombocytopenia [6]. There is no evidence suggesting the effectiveness of this mechanism in patients with thrombocytopathy resulting from ESRD.
The lack of improvement and even the limitation of PLT aggregation in TRAPtest in both groups in our study contradicted the hypothesis about the positive effect of fibrinogen supplementation on PLT function. The impaired aggregation indicated by TRAPtest following the ex vivo fibrinogen substitution was described by Hakimi et al. in patients undergoing cardiac surgeries. Adverse effects of fibrinogen supplementation on the aggregation of thrombocytes were also observed after the application of the combination of fibrinogen and PLT concentrate [33].
Thekkedath et al. observed a higher number of circulating fibrinogen fragments in patients with uraemia, which are responsible for the inhibition of thrombocyte aggregation. By binding to the GPIIb/IIIa receptor, they decrease the effectiveness of the fibrinogen-PLT complex [34]. Lovely et al. suggest an inhibiting role of the gammaA/gamma’ fibrinogen isoform which blocks the aggregation of PLT through the thrombin receptor [35].
The analysis of thromboelastometry results also allowed for the assessment of clot lysis. This is important from the perspective of the reports [36–38] on the increased risk of hyperfibrinolysis in patients with ESRD. We did not observe such cases in our study. This agrees with the study of Jalala et al., who reported that hypofibrinolysis is a prevalent phenomenon in patients with uraemia [23, 39]. This is one of the observations suggesting that there is an increased risk of thromboembolic events in such patients.
There are some limitations of this study. The groups were not homogenous and differed considerably in concerning patient age. The plasma activity of most known procoagulant factors increases with age, whereas anticoagulant factors (antithrombin, tissue factor pathway inhibitor, and protein C) and profibrinolytic factors (plasminogen and tissue plasminogen activator) do not significantly increase with age. Imbalance between procoagulant activity and anticoagulant and fibrinolytic activity increases in an age-dependent manner [40].
Patients with ESRD on HD constituted a heterogeneous group from the perspective of the aetiology of renal failure. Some of the diseases leading to ESRD may predispose to coagulation disorders to a greater extent, diabetic neuropathy is given as one example. Further studies should investigate the role of fibrinogen in modelling the inflammatory response, inter alia, by affecting the production of cytokines [41], this aspect was not discussed in our study. Furthermore, our study did not examine the impact of the vessel wall and endothelium on the coagulation process.
Because of the constraints of the equipment, only two tests were selected from the available GHA-POCT methods. However, the European guidelines on the management of major bleeding and coagulopathy following trauma recommend that thromboelastometry be used with impedance aggregometry in the diagnosis of haemostasis disorders [11, 12].
CONCLUSIONS
From the analysis of the results obtained using GHA-POCT regarding the haemostatic profile of patients with ESRD on chronic dialysis, it transpires that there are characteristic differences compared to healthy individuals. Contrary to standard laboratory testing, thromboelastometry allows for the global assessment of secondary haemostasis (plasma component, fibrinolysis). Because of limitations in the assessment of PLT function, a thorough assessment of primary haemostasis (PLT component) is feasible when using thromboelastometry in combination with impedance aggregometry which is designed to assess the PLT function.
Considering all the above, it may be stated that GHA-POCT methods are valuable instruments for the diagnosis of hemostasis disorders. They allow us to discover unique disorders for the study group which cannot be observed using standard laboratory testing.
The haemostasis profile of patients with ESRD shows the limited potential of PLT aggregation, with no improvement after in vitro fibrinogen supplementation.
The information provided above may be used in clinical practice for optimizing the management of patients on chronic dialysis given a high risk of bleeding, and an optimal haemostatic plan should be prepared.