







Introduction
Fixed orthodontic appliance therapy for a mean period of 16 months can lead to increased levels of nickel (Ni) and chromium (Cr) ions in the saliva of patients [1], which can be an uncomfortable experience and affect the quality of life [2]. Ni and Cr are metals commonly used in the structure of fixed orthodontic appliances, including bands, brackets, and wires [3, 4]. Nickel is the most common contact allergen [5, 6] affecting women in Europe and the USA [6]. Ni, as an allergen, can cause immunological sensitivity in a number of people receiving long-term orthodontics. The Cr ion can also cause dermatitis, asthma and adverse biological and cytotoxic effects [7]. Mineral analysis of hair is accepted as a meaningful indicator of chronic exposure to and ingestion of metals such as Ni [5], and the content of nickel in hair and nails correlates with that of blood [8, 9]. Analysis of elements in hair tissue provides a noninvasive biomarker of exposure [10]. Although Ni and Cr are known as allergenic and cytotoxic orthodontic metals, very few and controversial studies have assessed the effect of orthodontic treatment on their systemic levels reflected by their best biomarker of exposure, hair [11].
Aim
The aim of this meta-analysis was to investigate hair Ni and Cr levels in subjects undergoing fixed orthodontic treatment compared with controls without orthodontic treatment.
Material and Methods
Search strategy and study selection
The meta-analysis was designed based on the guidelines for the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [12]. A comprehensive search was done using the databases PubMed, Web of Science, Scopus, Cochrane Library, and ScienceDirect from 1983 to January 2018. We searched the databases by a combination of the terms “nickel”, “chromium”, “orthodontic” and “hair”. The studies were selected for assessment of the hair levels of nickel and/or chromium in patients undergoing fixed orthodontic treatment (cases) compared with controls in the English abstract. The studies included in the meta-analysis had to: (I) use a case-control design, (II) report Ni and/or Cr levels after orthodontic treatment, (III) report controls without orthodontic treatment, and (IV) report the fixed appliances (archwires, brackets, tubes and bands) with stainless steel and/or Ni-Ti materials. There were no exclusion criteria for the case-control studies included.
Data extraction
One author (M.S.) searched and two authors (M.S. & M.M.I.) reviewed independently the articles for relevant publications. We used a standard protocol and reporting form for data extraction from each publication including the first author’s name, the year of publication, the country in which the study was conducted, the number of the cases and controls, the duration of treatment, and the mean age/gender (%) of the cases and controls.
Quality assessment
To evaluate the study quality, a nine-star protocol was used on the basis of the Newcastle-Ottawa Scale (NOS) for case-control studies [13]. A high-quality study was a study with ≥ 7 stars.
Statistical analysis
To compare hair Ni and Cr levels in the cases compared with the controls, a random-effects meta-analysis was performed by Review Manager 5.3 (RevMan 5.3, The Cochrane Collaboration, Oxford, United Kingdom) using standard mean differences (SMDs) and 95% confidence intervals (CIs). Because the orthodontic treatment periods were different in the studies, we used the SMD. Heterogeneity among studies was evaluated with the Q and the I2 statistics. The results were defined as heterogeneous for p < 0.10 or I2 > 50% [14] and a p-value (2-sided) < 0.05 was considered statistically significant in this meta-analysis. Sensitivity analyses were further conducted in which one study was removed and the rest were analyzed to evaluate whether the results were affected statistically significantly. In addition, the publication bias was assessed by visual inspection of funnel plots and formal testing using Begg’s and Egger’s tests [15]. The units of measurement of hair nickel or chromium levels were μg/g dry hair mass.
Results
Literature search and study characteristics
Out of 38 studies in the databases searched, after removing duplication studies, 18 studies were screened (Figure 1). Nine studies were excluded because they did not have relevant data and therefore the full texts of 9 studies were evaluated for eligibility. Then, 3 studies were excluded with reasons (2 studies were cross-sectional, and 1 study had two intervention groups without a control). Finally, 6 studies were included in the meta-analysis.
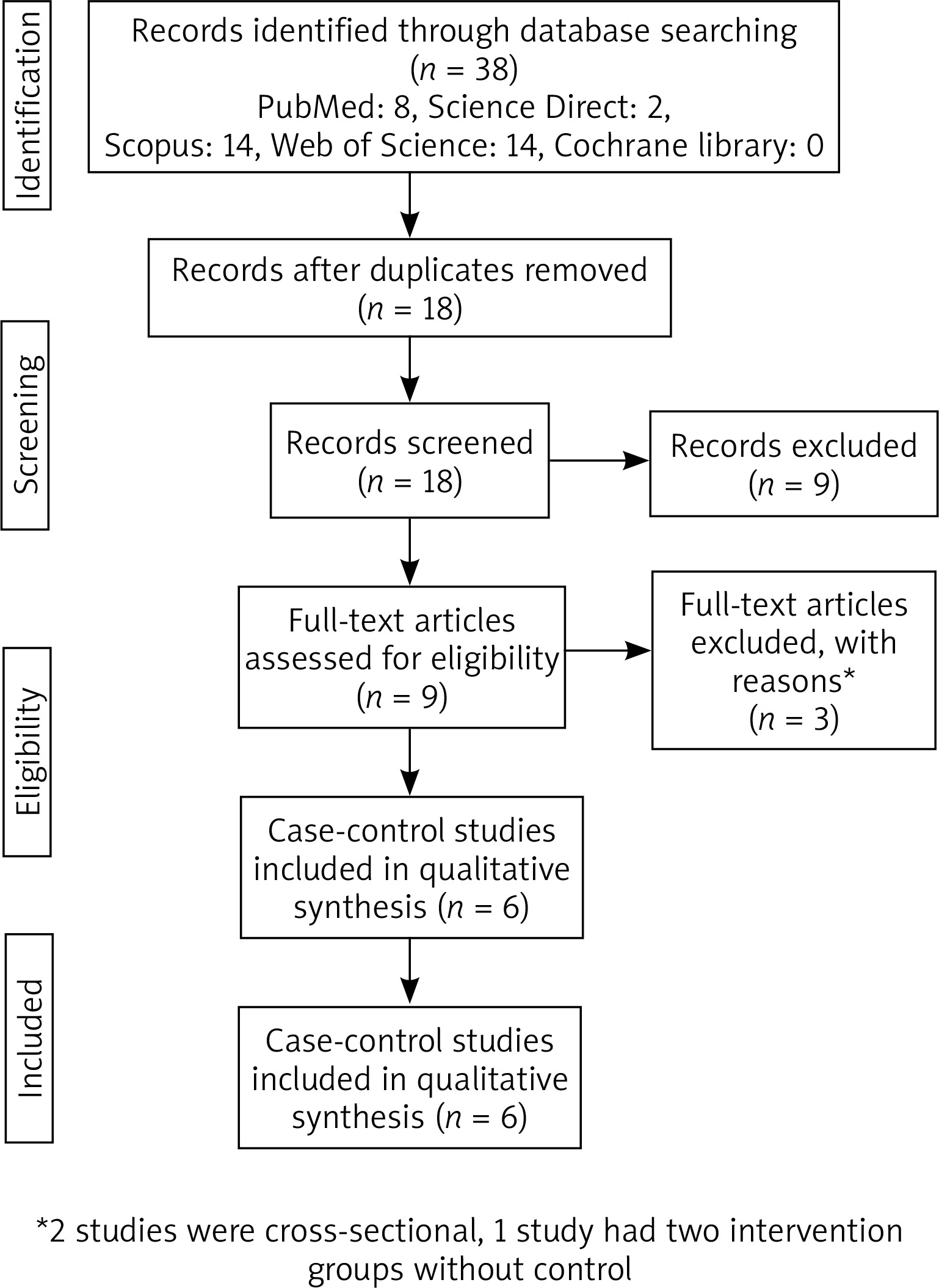
Table 1 shows the characteristics of the 6 studies included in the meta-analysis. The studies were published from 2006 to 2018. Two studies were reported from Poland [16, 17], 2 studies from Iran [3, 5], 1 study from Spain [18], and 1 study from Italy [19]. The study included 197 cases and 173 controls. The orthodontic treatment period was from 4 to ~ 69.8 months.
Table 1
Characteristics of studies included in the meta-analysis (n = 6)
| Reference (first author, year) | Country | No. of patients | No. of controls | Mean age [year]/male (%) of patients | Mean age [year]/male (%) of controls | Orthodontic treatment period [months] |
|---|---|---|---|---|---|---|
| Levrini, 2006 [19] | Italy | 15 | 15 | 18.9 (range: 10–25)/0 | Matched/matched | – |
| Mikulewicz, 2011 [16] | Poland | 28 | 18 | Matched/ matched | Matched/matched | Mean: 18–24 |
| Abtahi, 2013 [5] | Iran | 24 | 24 | Range: 12–20/0 | Range: 12–20/0 | 4 |
| Martín-Cameán, 2014 [18] | Spain | 70 | 56 | –/34.3 | –/42.8 | ~24 |
| Mikulewicz, 2015 [17] | Poland | 36 | 32 | –/– | –/– | ~69.8 |
| Jamshidi, 2018 [3] | Iran | 24 | 28 | 17.54/29.2 | 15.42/53.8 | 12 |
Standard mean differences of Ni and Cr levels between cases and controls
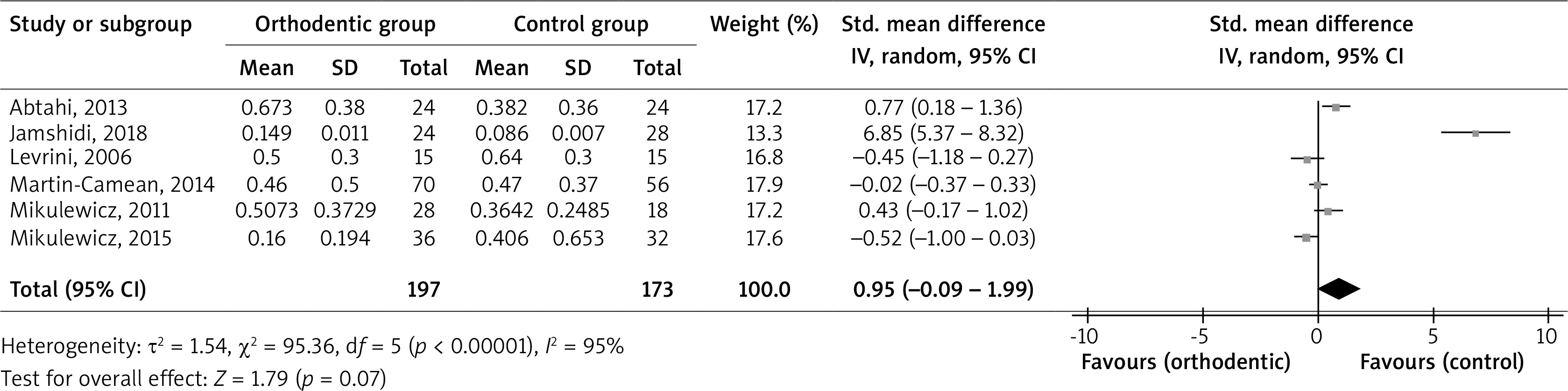
The pooled SMD of hair Ni levels between the cases and controls was 0.95 µg/g (95% CI: –0.09, 1.99; p = 0.07; I2 = 95%; pheterogeneity < 0.00001); the result showed that the Ni level was similar in the cases compared with the controls, but with a slightly elevated level in the cases (Figure 2). To reduce heterogeneity (sensitivity analysis), we removed 1 study [3] from the analysis so that pooled SMD became 0.04 µg/g (95% CI: –0.41, 0.49; p = 0.87; I2 = 72%; pheterogeneity = 0.006); the result showed again that the Ni level was similar in the cases compared with the controls.
Figure 2
Forest plot of random effects of hair nickel levels in patients undergoing fixed orthodontic treatment compared with controls
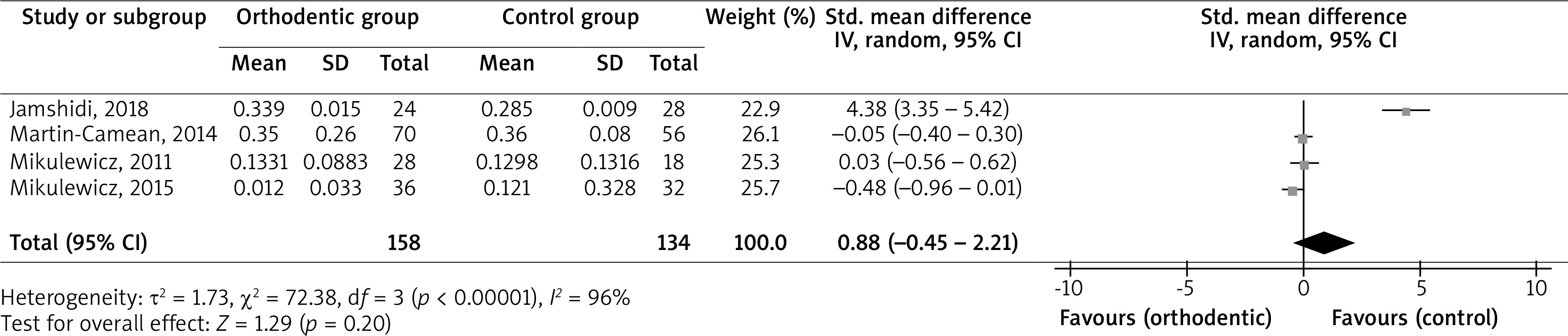
The result of the pooled SMD of hair Cr levels between the cases and controls was 0.88 µg/g (95% CI: –0.45, 2.21; p = 0.20; I2 = 96%; pheterogeneity < 0.00001). Therefore, the Cr level was similar in the cases compared with the controls, but with a slightly elevated level in the cases (Figure 3). To reduce heterogeneity (sensitivity analysis), we removed 1 study [3] from the analysis so that the pooled SMD became –0.16 µg/g (95% CI: –0.45, 0.13; p = 0.28; I2 = 18%; pheterogeneity = 0.30); the result showed that the Cr level was similar in the cases compared with the controls.
Quality assessment
Study-specific quality scores are summarized in Table 2. The mean score was 7. Four case-control studies were awarded ≥ 7 stars and defined as high-quality studies.
Table 2
Quality of case-control studies included in the meta-analysis (n = 6)
| Reference (first author, year) | Adequate definition .of cases* | Representativenessof cases* | Selection of control subjects* | Definition of control subjects* | Control for important factor or additional factorΔ | Exposure assessment* | Same method of ascertainment for all subjects* | Nonresponse rate• | Total quality scores |
|---|---|---|---|---|---|---|---|---|---|
| Levrini, 2006 [19] | * | * | – | – | ** | * | * | * | 7 |
| Mikulewicz, 2011 [16] | * | * | – | * | ** | * | * | * | 8 |
| Abtahi, 2013 [5] | * | * | * | * | ** | * | * | – | 8 |
| Martín-Cameán, 2014 [18] | * | * | – | * | – | * | * | * | 6 |
| Mikulewicz, 2015 [17] | * | * | * | – | – | * | * | * | 6 |
| Jamshidi, 2018 [3] | * | * | * | * | * | * | * | – | 7 |
| Mean score | 7 | ||||||||
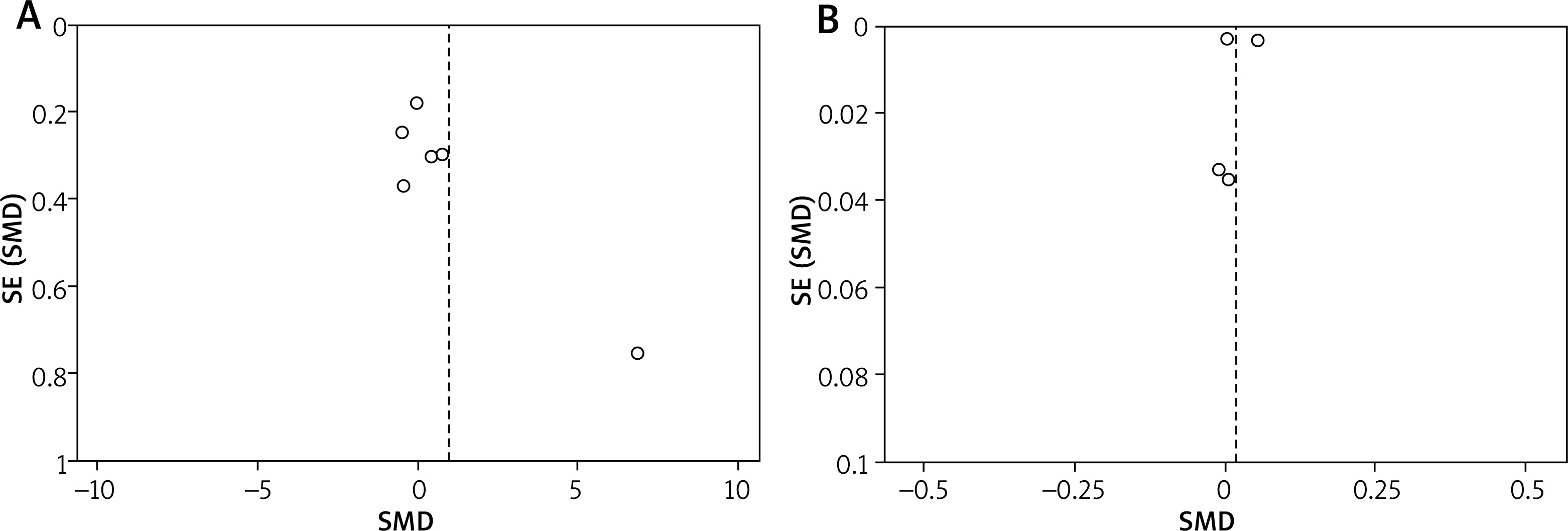
Publication bias
Figure 4 shows the funnel plot of studies included in two analyses. Begg’s test did not reveal, but Egger’s test did reveal, significant evidence of publication bias among the included studies (Figure 4 A) for reporting Ni level, whereas Begg’s and Egger’s tests did not reveal significant evidence of publication bias among the included studies based on sensitivity analysis and removing one study [3]. Begg’s and Egger’s tests did not reveal significant evidence of publication bias among the included studies for reporting Cr level (Figure 4 B) and also among the included studies based on sensitivity analysis and removing one study [3].
Discussion
Corrosion of orthodontic appliances and metal ion release in the environment of the oral cavity are recognized as two main factors for metal ion release [17]. This meta-analysis evaluated hair Ni and Cr levels in subjects undergoing orthodontic treatment compared with controls. The results showed that levels of both metals were higher in the patients, but these differences were not significant even with regard to sensitivity analysis. In addition, the increase in Ni level was greater than the increase in Cr level, when compared to the controls. Out of six studies in the meta-analysis including hair Ni levels, three studies [3, 5, 16] showed higher hair levels of Ni in the patients and the other studies [17–19] showed lower levels. Also, out of five studies including Cr levels, two studies [3, 16] reported higher hair levels of Ni of the cases and the other studies [17, 18] reported lower levels. Among all studies, only the study of Jamshidi et al. [3] showed significant differences in Ni and Cr concentrations between the two groups and reported that due to the slightly elevated levels of Ni and Cr ions in hair of patients undergoing fixed orthodontic treatment the cytotoxic and allergic effects of these ions can be considered. Pazzini et al. [20] suggested that nickel can affect inflammatory reactions throughout orthodontic treatment. Therefore, considering ion levels in future studies may be necessary.
After 6-month orthodontic treatment compared with before treatment, Amini et al. [11] demonstrated that hair Ni and Cr levels increased by 381 and 16%, respectively. Mikulewicz et al. [21] reported increases of 39 and 2.5% in Ni and Cr levels, respectively, of scalp hair after orthodontic treatment compared with before treatment, without a significant difference. Abtahi et al. [5] observed that after 4-month treatment Ni changes in the scalp hair of patients undergoing fixed orthodontic treatment increased to 190%. A 6-month trial with fixed orthodontic appliances consisting of either metal injection molding or conventional brackets [22] showed that hair nickel and chromium levels increased by about 200% and 185%, respectively. Some shampoos and many hair perm dye bleach products transfer Ni into the hair [5].
High metal ion levels in saliva were found 1 to 2 weeks after exposure to metal appliances and then these reverted to the initial levels [4, 23]. Orthodontic appliances release ions into the oral environment [24, 25] more intensely in the first months of appliance placement [24–26]. In the studies included in the meta-analysis, one study [5] after 4 months’ and another study [9] after 12 months’ orthodontic treatment had higher Ni levels of hair in the cases compared with the controls, whereas another study [17] after around 69.8 months’ orthodontic treatment had higher levels in the controls compared with the cases. Jamshidi et al. [3] in 12 months’ treatment observed higher Cr levels in the cases compared with the controls, whereas Mikulewicz et al. [17] after around 69.8 months’ orthodontic treatment had the opposite result. Therefore, long-term treatment reduced hair levels of these ions, which may be because of reducing ions released into the oral environment. The treatment period in the study of Abtahi et al. [5] was 4 months, whereas in the study of Mikulewicz et al. [17] it was around 69.8 months, and the hair Ni level in the first study was higher than in the second study.
One study [10] evaluated the role of age and sex on hair Ni and Cr levels before orthodontic treatment that the results showed that there was no significant difference between the genders or between age < 18 and > 18 years. Martín-Cameán et al. [18] reported that females had higher metal levels in the cases undergoing orthodontic treatment compared with the controls, but no significant associations were found between age and metal levels in both groups.
Overall the results indicated that hair Ni level changes were greater than Cr level changes after treatment, especially in the subjects undergoing orthodontic treatment compared with the controls. In addition, there were different results between studies, which may be because of differences in conditions of the hair collection, treatment periods, and gender. In one study [18] the hair was washed by ultrasonic cleaning, but in another study [16] it was washed with a proprietary baby shampoo under laboratory conditions and then with water. The hair Ni level in the first study was less than the second study. In addition, two studies [5, 19] conducted the analysis on women and three other studies [3, 16, 18] included both genders, and the results of ion analysis were different between them.
There were several significant weaknesses in the meta-analysis. First, duration of treatment and measurement methods were different in the studies. Second, age and sex were not matched between the groups. Finally, there was a low number of participants in most studies.
Conclusions
Due to the slightly elevated hair levels of Ni and Cr in the subjects undergoing fixed orthodontic therapy, changing the components of fixed orthodontic appliances can be considered as an acceptable solution in the future. Therefore, future studies need to assess the levels of these ions in serum and saliva of patients for more accurate confirmation of cytotoxic and allergic effects after fixed orthodontic therapy.