





Postoperative pain associated with hip replacement surgery can be severe, decreasing the patient’s mobility and satisfaction with perioperative treatment [1, 2]. Regional techniques are commonly used as anesthesia and postoperative analgesia in hip surgery patients [3]. However, some regional procedures can affect patients’ ambulation and prolong their hospital stay. Moreover, central regional blocks, such as spinal and epidural techniques, also immobilize the contralateral to the surgical side lower limb [4].
In recent years, investigators have introduced many novel regional anesthesia techniques performed under ultrasound control. Among them, the erector spinae plane block (ESPB), invented by Forero and colleagues [5] in 2016, has been the most successfully used in clinical practice. We conducted several trials concerning ESPB in patients undergoing cardiac and breast surgery [6–9]. In these studies, we found that this novel block performed at the thoracic level reduced postoperative opioid consumption.
In the current study, we investigated the role of the lumbar ESPB compared to epidural analgesia in patients undergoing primary hip replacement surgery. The main outcome of our study was postoperative opioid consumption; the others included pain severity and the patient’s ability to ambulate.
METHODS
This was a prospective, single-center pilot study. The study obtained a positive opinion from the Local Ethics Committee of the Medical University of Lublin. Written informed consent was obtained from each patient, and the study was conducted following the tenets of the Declaration of Helsinki for medical research involving human subjects.
We included consecutive patients scheduled for primary hip replacement surgery due to coxarthrosis, aged > 18 and < 100 years, anesthetized with spinal technique. We excluded people who were allergic to the studied drugs; took painkillers not related to coxarthrosis; had active cancer, dementia, or challenging contact with the patient; suffered from depression or other psychiatric disorders that required antidepressant treatment; alcohol or recreational drug addiction; and had contraindication to the regional block.
Anesthetic intervention
Before the induction of anesthesia, we admini-stered 4 mg of dexamethasone and ondansetron intravenously (i.v.). All patients received subarachnoid anesthesia. We performed spinal anesthesia in the patient’s lateral position with the operated hip down. We used 0.5% bupivacaine (Marcaine Heavy Spinal) with fentanyl (5 mg mL–1) and a 25–27 G pencil point spinal needle. Then, we allocated patients to two groups according to the interventions (computer-generated randomization). We performed ESPB in the first group (the ESPB group), whereas patients in the second group had epidural analgesia (the epidural group). Both techniques were applied after spinal anesthesia.
We performed the lumbar ESPB under ultrasound control at the L3 level on the ipsilateral site of the surgery. After dissection with 0.9 NaCl, we left a catheter in the ESP. Then, we used 0.25% bupivacaine with epinephrine (5 mg mL–1), 0.4 mL per kg, up to 40 mL. We performed epidural analgesia using a combined technique (Espocan, B. Braun). Through an epidural catheter we applied a test dose of 2% lidocaine (2 mL). At the end of the surgery, the patient received 5 mL of a mixture containing 0.1% bupivacaine with fentanyl (2 mg mL–1). Moreover, we administered 5 mg of oxycodone i.v. in both studied groups.
Postoperative pain control
We treated pain with the abovementioned mixture of bupivacaine and fentanyl in a constant flow of 5 mL h–1. Moreover, each participant received a pump with oxycodone (1 mg mL–1) using a patient-controlled analgesia (PCA) technique, a bolus of 1 mL, and a lockout of 5 minutes. Patients also received metamizole, 1 g, every six hours, i.v. In the case of pain ≥ four on the visual analog scale (VAS), the patient received a bolus of bupivacaine mixture (5 mL). Patients also obtained i.v. paracetamol (four times a day) and ondansetron (4 mg, twice daily).
Outcomes
The primary outcome in our study was total oxycodone consumption with PCA during the first 24 postoperative hours.
The other measured outcomes included all PCA demands and measuring pain on the VAS. We measured pain at rest and upon activity before the surgery, after transfer to a postoperative unit, as well as 4, 8, 24, and 48 hours following the surgery.
A physiotherapist evaluated the patient’s ability to sit, stand upright, and walk at planned time points. The physiotherapist also assessed the quadriceps femoris’ muscle strength on the side of the hip replacement and the contralateral flank. We used the six-grade Lovett scale to measure muscle strength, in which 0 denotes no muscle contractility, and 5 denotes the complete range of motion against gravity, with full resistance [10]. Moreover, the physiotherapist used the Timed Up and Go test (TUG) [11]. In the TUG test, we measured the time the patient took to rise from a chair, walk three meters, turn around 180 degrees, walk back to the chair, and sit down while rotating 180 degrees. We assessed the patient before the surgery as well as 24 and 48 hours after hip replacement.
We measured the patient’s systemic blood pressure (BP), heart rate (HR), and respiratory rate during pain evaluation. On the first postoperative day, we assessed the patient’s satisfaction and quality of recovery (QoR) through the QoR-40 questionnaire [12]. We used the QoR-40 in our previous study [9].
Statistical analysis
We analyzed continuous variables with the t-test or the Mann-Whitney U test. We checked the distribution of the data through the Shapiro-Wilk test. We used mean and standard deviations (SD) for demographics, means and confidence intervals (CI) for normally distributed parameters, medians and interquartile ranges (IQR) for non-normally distri-buted parameters, and numbers and percentages to present categorical data. All measurements were performed using Statistica 13.1 software (Stat Soft. Inc., Tulsa, OK, United States).
RESULTS
We recruited 23 participants: 12 for the epidural group and 11 for the ESPB group. Patient demographics are presented in Table 1.
TABLE 1
Patient demographics
We found that patients in the epidural group used less oxycodone via the PCA pump (9.1 mg (5.2–13.0) (CI)) than participants in the ESPB group (15.5 mg (9.8–21.3), P = 0.049) (Figure 1). Patients in the ESPB group had more demands with PCA than participants in the epidural group (10.5 [6–16] [IQR] vs. 25 [16–51], P = 0.016). Five patients in the ESPB group and five patients from the epidural group received an additional bolus of bupivacaine mixture according to the study protocol (P = 0.85). As presented in Table 2, we found no difference between the studied groups in most outcomes. Moreover, we did not note discrepancies in the patient’s ability to sit, stand upright, and walk. Only a single patient in the ESPB group had nausea and vomiting. We found higher heart rates in the epidural group at admission (77 (72–83) (CI) vs. 69 (65–73), P = 0.02), at 24 hours (80 (75–85) vs.72 (68–76), P = 0.01), and at 48 postoperative hours (79 (75–83) vs. 70 (66–74), P = 0.003).
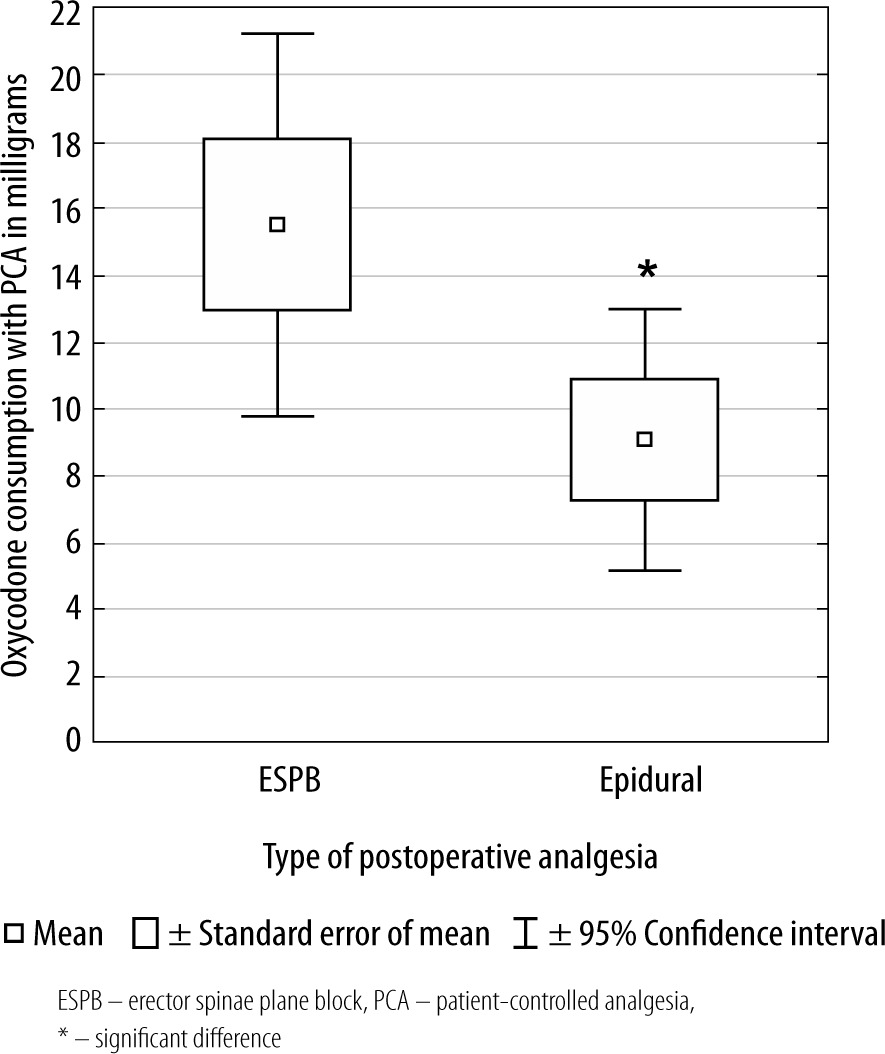
TABLE 2
Outcomes
[i] IQR – interquartile range, Lovett CS – Lovett measurement on contralateral side, Lovett OS – Lovett measurement on operated side, PACU – postoperative care unit, QoR-40 – quality of recovery, QoR-40 A and B – QoR-40 part A and B, VAS – visual analog scale, VAS R – VAS at rest, VAS A – VAS upon activity, TUG – the Timed Up and Go test
DISCUSSION
The results of this study suggested that the ESPB is equivalent to epidural analgesia in most studied outcomes in patients undergoing hip replacement surgery. The only differences noted between our groups were the higher consumption of oxycodone (Figure 1) and the more demands for PCA pump among ESPB patients. However, higher opioid consumption did not affect nausea and vomiting. We did not find discrepancies in pain, quality of recovery, muscle strength, and the TUG test between the two groups. The significant difference in HR between the studied groups at 24 and 48 hours postoperatively was like the HR results noted at admission.
To our knowledge, no previous research has directly investigated the lumbar ESPB and epidural analgesia. However, Elshazly et al. [13] compared the ESPB to caudal block in children undergoing hip and proximal femur surgery. In this randomized controlled trial (RCT), the authors noted lower pain severity and the time to first rescue analgesia in patients following caudal block. In contrast to our study, Elshazly et al. [13] used a single-injection technique without leaving a catheter for continuous postoperative infusion.
Moreover, Townsend et al. [14] found that following the lumbar ESPB, patients had lower opioid consumption with PCA at 8 hours postoperatively than the control group. The authors of this study did not find differences in opioid consumption at 24 and 48 hours after the operation and pain severity between the studied groups. However, they did not evaluate the patients’ ambulation.
In the current study, we hypothesized that the ESPB could hasten ambulation more effectively than the epidural technique. Our previous study showed that the continuous femoral nerve block was superior to the adductor canal block in pain reduction [10]. However, patients following the adductor canal block had better mobility and quadriceps femoris muscle strength, measured with Lovett’s scale. The results of the current study did not show any difference in the advantage of the ESPB according to the patient’s ambulation.
Our study has some limitations. We did not randomize participants to the studied groups. Our cohort was relatively small and included only 23 patients. Although we obtained statistically significant differences in some points, further studies are necessary to confirm these results.