





Coronavirus disease, known as COVID-19, is an infectious disease caused by SARS-CoV-2, the first outbreak of which occurred in the Chinese city of Wuhan in December 2019. The first case in Poland was confirmed on March 4, 2020 in a person returning from abroad. In September 2020, the number of SARS-CoV-2 infections worldwide exceeded 30 million and nearly one million people died.
The most important clinical symptom of COVID-19 is severe pneumonia, which leads to acute respiratory distress syndrome (ARDS). Therefore, the affected patients require the implementation of invasive mechanical ventilation techniques in the intensive care unit (ICU).
In addition to severe respiratory failure, haemostasis disorders are one of the essential factors affecting the treatment and worsening the prognosis [1, 2].
Analysis of the results of studies in patients treated for COVID-19 has demonstrated hypercoagulability [3, 4] resulting from overactivation of cytokines – called a cytokine storm – in the course of an acute inflammatory response associated with SARS-CoV-2 infection. In such cases, pulmonary endothelial dysfunction is observed, particularly severe in the alveolar capillaries [5].
The most common changes in the coagulation tests include prolonged coagulation times (activated partial thromboplastin time – APTT, prothrombin time – PT and thrombin time – TT) as well as high concentrations of fibrinogen and D-dimer [6].
Although some of the above changes are similar to those observed in disseminated intravascular coagulation (DIC), many authors highlight that the coagulation disorders in COVID-19 patients are diverse and difficult to be classified in an explicit manner [7].
The aim of the present study is to characterise the haemostatic profile of patients hospitalised in the Intensive Care Unit of the Hospital for Infectious Diseases (HID) in Warsaw based on the assessment of clotting parameters, risk of thromboembolic complications and severity of patients’ general conditions.
METHODS
The study design was submitted to the Bioethical Committee of the Medical University of Warsaw (no opinions are given in the case of retrospective studies).
The retrospective analysis involved the first 10 adult patients hospitalized in the ICU of the HID in Warsaw in the second quarter of 2020. Patients were referred for ICU admission due to respiratory failure associated with SARS-CoV-2 infection, which was confirmed by the real-time PCR assay. One patient was excluded from the analysis as he died within the first hour of ICU hospitalization and the diagnostic procedures of the haemostatic system were unfeasible.
Ultimately, the medical records of nine patients were analysed covering the period between ICU admission and discharge or death. One patient was admitted from the emergency department; the others were earlier hospitalised in the medical departments of the HID. The decision about ICU admission was made based on the criteria described in the ICU admission protocol developed by the national consultant on anaesthesiology and intensive care.
All patients admitted to the ICU presented respiratory failure, met the ARDS criteria according to the Berlin definition [8] and required invasive mechanical ventilation, which was carried out in accordance with the ARDSNet recommendations [9].
During treatment, various analgosedation strategies were used – with propofol, midazolam, fentanyl, dexmedetomidine. In cases of heart failure, intravenous infusions of catecholamines (norepinephrine, dobutamine, adrenaline) were administered.
Demographic, clinical and laboratory parameters as well as hospitalisation times prior to ICU admission were analysed.
During the first day of ICU hospitalization, a panel of laboratory tests was routinely performed, including complete blood counts, biochemistry, coagulogram. When assessing the haemostatic profile, the following were analysed in detail:
The severity of patients’ conditions was assessed with SAPS II, APACHE II and SOFA scores; the Optimed calculators were used.
Methods of assessing haemostasis disorders on ICU admission and determination of the risk of thromboembolic complications
Besides thrombocytopaenia, the statistically most common coagulopathy in ICU patients with sepsis is disseminated intravascular coagulation (DIC) [10]. In its advanced form, it is a systemic, uncontrolled activation of the coagulation system, leading to multi-organ failure resulting from organ perfusion disorders [11].
To assess the incidence of DIC in the COVID-19 pneumonia group, the authors used the scale developed by the International Society on Thrombosis and Haemostasis (ISTH) in 2009 (Table 1).
TABLE 1
The diagnostic algorithm for acute disseminated intravascular coagulation (DIC) [12–14]
In 2017, Iba et al., who analysed 1498 patients, suggested a new definition of early coagulopathy in sepsis [15]. According to the authors, the intermediate stage between the initial activation of the coagulation system during the infection and acute fully symptomatic DIC is sepsis-induced coagulo-pathy (SIC). The above definition was used in some other studies performed over the next years [11, 16].
In addition to the INR and platelet count, the SIC scale includes a modified SOFA score assessing the performance of the respiratory, circulatory, hepatic and renal systems. The dysfunction of each of them is scored one, and no more than two points when two or more systems have failed. Therefore, the maximum modified SOFA score does not allow to diagnose SIC (four points or more). A prerequisite is the occurrence of organ failure together with INR and PLT abnormalities [15]. The diagnostic criteria for SIC are presented in Table 2.
TABLE 2
The diagnostic algorithm for sepsis-induced coagulopathy (SIC) [15]
| Parameter | 0 | 1 | 2 |
|---|---|---|---|
| INR | ≤ 1.20 | 1.21–1.40 | > 1.40 |
| Platelet count (G L–1) | ≥ 150 | 100–149 | < 100 |
| Modified SOFA | 0 | 1 | ≥ 2 |
Irrespective of the aetiology and location of infection, ICU hospitalisation is associated with an increased risk of thromboembolic complications [17]. Therefore, the Padua prediction score was used in each patient admitted to the ICU (Table 3).
TABLE 3
The Padua score used to assess the risk of deep vein thrombosis or pulmonary embolism in hospitalised medical patients [18]
Statistical analysis
Statistical analysis was performed using the Po-lish version of Statistica 13.0 software (Tibco, Palo Alto, USA). Descriptive statistics were used to summarise the data. The Shapiro-Wilk test was applied to verify the normality of distribution. Categorical variables were presented as numbers and percentages.
RESULTS
The laboratory results of all patients (7 men and 2 women aged 27-84 years) were analysed. The detailed characteristics of patients were presented in Table 4.
TABLE 4
Characteristics of patients admitted to the ICU of the Hospital for Infectious Diseases in Warsaw
All patients required invasive mechanical ventilation and 7 patients received a continuous infusion of catecholamines due to circulatory failure.
In all patients, the Padua prediction score was found to be ≥ 5, which indicated a high risk of thromboembolic complications. The lowest score was observed in two out of three survivors (Table 5).
TABLE 5
Scores on ICU admission according to the scales used and deaths in the study group
Fulfilling the criteria for acute disseminated intravascular coagulation
In most patients, the platelet count remained within the upper reference limit. None of the nine patients presented severe thrombocytopaenia (< 50 G L–1) on ICU admission. Mild thrombocytopaenia (100–150 G L–1) was observed only in one patient during the first 24 hours of ICU stay. During the entire period of ICU hospitalization, thrombocytopaenia was not found in any of the three survivors (Figure 1A).
FIGURE 1
A) Consecutive determinations of platelet counts performed in each patient during ICU hospitalisation. B) Consecutive determinations of D-dimer levels performed in each patient during ICU hospitalisation. C) Consecutive determinations of prothrombin times during ICU hospitalisation. D) Consecutive determinations of fibrinogen levels during ICU hospitalisation
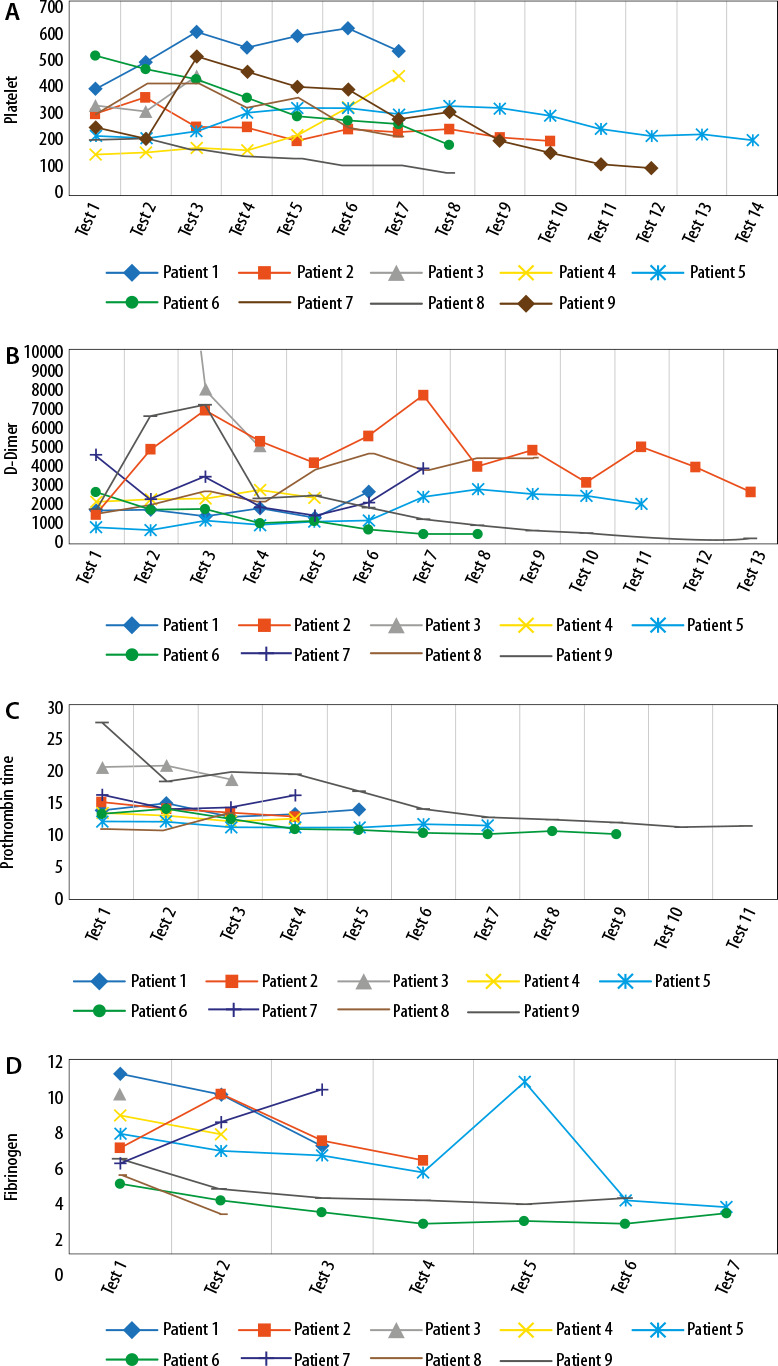
On ICU admission, each patient had an elevated (> 500 ng mL–1) D-dimer level, which was normalized in one patient on hospitalisation day 10 (Figure 1B). A significant increase (> 4000 ng mL–1) was detected in the majority of patients. Such an increase was not observed in any of the three survivors discharged from the ICU (Figure 1B).
A significant prolongation in PT by 3 seconds above the upper reference limit was observed in two patients within the first day of ICU hospitalisation (Figure 1C).
None of the patients showed hypofibrinogenae-mia (Figure 1D), which is a typical component of coagulopathy in acute DIC.
The results of the study patients did not allow to diagnose acute DIC based on the established criteria (Table 5).
Fulfilling the sepsis-induced coagulopathy criteria
On ICU admission, none of the patients fulfilled the criterion for SIC, although the majority of patients had maximum modified SOFA scores (Table 5). The above resulted from the fact that organ changes were not accompanied by adequate deviations in coagulation tests. In addition to respiratory failure observed in all patients admitted to the ICU, the second most common condition was circulatory failure.
DISCUSSION
Patients with advanced stages of COVID-19 requiring ICU hospitalization are characterized by progressive respiratory failure, which shortly leads to severe ARDS. Based on clinical observations of COVID-19 and laboratory results, the disorders of gas exchange in the lungs were considered to be associated with coagulopathy, which was confirmed by autopsy findings. One of the key manifestations was the presence of pulmonary microemboli [7, 11]. Therefore, assessment of the risk of thromboembolic complications and careful monitoring of the coagulation system were found essential for the diagnosis and treatment of patients with SARS-CoV-2 infection.
The laboratory findings of the study patients disclosed that the main coagulation disorders were high levels of D-dimer and fibrinogen, which were higher than the upper reference limit in 100% and 77% of patients, respectively. The above results are consistent with some other literature data describing coagulopathies in COVID-19 patients [6, 11].
During ICU hospitalisation, the study group of patients presented a normal or only slightly reduced platelet count, which is in line with the findings reported by Maquet et al. who analysed 263 patients with COVID-19 in the European population. Thrombocytopaenia, mainly mild, was observed in only 24.9% of them [19].
The above results are inconsistent with the early reports based on observations of COVID-19 patients treated in China, indicating substantially higher incidences of thrombocytopaenia (up to 72.7%) [20, 21].
It is difficult to explain the discrepancies described. One possible hypothesis is that Chinese reports concerned the beginning of 2020, i.e. the early stage of pandemic when knowledge of diagnosis and management was limited, diagnoses were delayed and involved patients with more advanced stages of COVID-19 and secondary coagulopathy; in many cases, patients who already fulfilled the criteria of fully symptomatic acute DIC. Similar differences between the studies in Chinese and European populations regarded prolonged clotting times, especially PT [2, 22].
It can be assumed that the knowledge and experience gained in the following months of the SARS-CoV-2 epidemic enabled earlier diagnoses and implementation of multidirectional therapy (antithrombotic prophylaxis, antiviral and anti-inflammatory treatment), which reduced the incidence of increased consumption coagulopathy characteristic of acute DIC occurring during multi-organ failure in patients with septic complications of COVID-19.
Since thrombocytopaenia and prolonged PTs were not universally observed in the analysed group, the concept that coagulopathy in COVID-19 patients takes the form of SIC was also not confirmed.
Considering all the disorders found, it seems that patients infected with SARS-CoV-2 are likely to develop some previously unknown pattern of coagulopathy, i.e. COVID-19-associated coagulopathy (CAC), observed more often than acute DIC or SIC [23]. The characteristic elements of CAC include [11, 23]:
high concentrations of D-dimer and fibrinogen,
lack of prolonged coagulation times,
lack of severe thrombocytopaenia,
higher incidences of thromboembolic complications, as compared to haemorrhagic complications.
According to current data, thromboembolic complications are observed in 16-49% of COVID-19 patients admitted to the ICU [24]. It is therefore important to ensure optimal anticoagulant therapy, as reflected in the current guidelines and recommendations for the diagnosis and treatment of COVID-19 patients [25, 26].
The Padua scores in the study group of patients indicate a high risk of thromboembolic complications, which is consistent with the data reported by other authors, suggestive of a prothrombotic haemostatic profile in patients with COVID-19 [27–29]. Based on the above, the therapeutic regimens were developed involving early and widespread thromboprophylaxis [30, 31].
According to Klok et al., however, despite the use of low-molecular-weight heparins in all patients with COVID-19, the incidence of thromboembolic events was still as high as 31% [32].
The above findings may be explained by the results reported by Tang et al. According to them, the use of low-molecular-weight heparins has translated into a reduction in 28-day mortality only in the most severely ill patients (D-dimer > 6 times the upper limit of normal) [31]. Therefore, it can be concluded that in the remaining patients the heparin therapy has not been effective in reducing mortality.
With such high levels of D-dimer as the only indication for anticoagulant therapy, the use of this kind of therapy would be limited to a narrow group of patients. This is confirmed indirectly by the results of our study, in which only 3 patients would meet the above criterion on ICU admission.
According to the reports on management of COVID-19 patients available in literature, there is no comprehensive and generally accepted regimen to reduce the effects of thromboembolic complications on the clinical course of SARS-CoV-2 infection. Studies are currently underway to assess the effectiveness of widespread use of therapeutic doses of low-molecular-weight heparins, fibrinolytics or antithrombin III, yet we still have to wait [33–35] for explicit results of studies in large populations of patients.
Our study has many limitations. Due to its retrospective nature and a relatively small group of patients included, the results presented by us cannot be considered relevant to possible modifications of already existing therapeutic strategies or the development of new strategies. Nevertheless, it confirms the reports suggesting a newly defined phenotype of coagulopathy (CAC) in COVID-19 patients hospitalized in the ICU. Moreover, to the best of our knowledge, our study is the first attempt to characterize the haemostatic profile in COVID-19 patients hospitalized in the ICU in the Polish population.
CONCLUSIONS
The haemostatic profile in patients treated for pneumonia caused by SARS-CoV-2 infection is characterised by a complex diagnostic and clinical picture that has not been described before the epidemic. This picture cannot be explicitly assigned to DIC or SIC conditions common in sepsis patients.
In view of incomplete knowledge of the pathophysiology of coagulopathies, the currently available recommendations should be followed, which advocate regular monitoring of the coagulation system, including levels of D-dimer and fibrinogen, PT times and platelet counts as well as widespread use of anticoagulant prophylaxis [30, 36].
The question that remains to be answered is whether the changes observed in the haemostatic system result only from a severe systemic inflammatory response or are also associated with the specific features of SARS-CoV-2.