





Complications related to airway management rarely occur in operating theatres; however, these complications may cause life-threatening situations [1]. Qualitative and quantitative analysis from the Fourth National Audit Project (NAP4) of the Royal College of Anaesthetists and Difficult Airway Society shows major airway complication prevalence in the United Kingdom [2, 3]. The NAP4 adds valuable information to anaesthesia practice. However, one of the limitations of NAP4 is being only a reflection of practices in one country. Therefore it cannot be extended to other countries. Additionally, Cook and MacDougall-Davis [4] noted that it was hard to measure practical differences for the application of the NAP4 in other countries. This prospective observational cohort study was planned to identify airway-related complications in a Polish university hospital. The primary outcome of this study was to determine the prevalence of airway management complications. The secondary outcome was to determine the main causes of related complications.
METHODS
After Ethics Committee approval (KOU-GAEK: 2018/15), the study was registered at Clinical trials. gov (NCT03550326). This study is designed as a prospective cohort study. Adult patients undergoing elective surgery under general anaesthesia within the period of January–July 2018 were included in the study. Demographic data, mask ventilation score, American Society of Anesthesiologists (ASA) physical status, Mallampati and Cormack-Lehane scores, type of devices used in airway management, and complications were recorded. The Han grading scale for mask ventilation (ventilation score) was used [5]. The researchers were present as observers during the airway management, including anaesthesia induction and the recovery period. They were not involved in the anaesthesia procedure. Patients undergoing emergency surgery were excluded, as well as those who received regional anaesthesia.
The observed airway problems included hypoxemia, need for rescue airway device, oesophageal intubation, difficult airway management, inappropriate tracheal tube selection, cervical immobilization, post-traumatic anatomy, small mouth opening, technical problems, ventilator-related problems, disconnection of breathing system, accidental extubation, malpositioning of supraglottic airway devices (SAD), tachycardia (defined as a heart rate > 100 beat min−1) and hypertension (based on a definition of blood pressure > 140/90 mm Hg).
Complications were divided into four categories based on severity:
Without any permanent problem.
Mild complications (lip injury, teeth damage).
Moderate complications (airway obstruction, pulmonary aspiration).
Severe complications (urgent surgical airway intervention, admission to intensive care unit, irrevocable brain damage, death).
Oxygen saturation (SpO2) below 93% was defined as hypoxemia [6]. Patients intubated after multiple attempts during difficult intubation were considered as multiple intervention cases if there was a difficult SAD placement [7]. Urgent surgical airway intervention included needle and surgical cricothyroidotomy or surgical tracheostomy.
The SPSS 22.0 program was used for statistical analysis. Mean, standard deviation, median, lowest and highest values, frequency and ratio values were used for descriptive analysis of the data. Variable distribution was measured with the Kolmogorov-Smirnov test. The Mann-Whitney U test was applied for quantitative independent data analysis. The χ2 test was used for qualitative independent data analysis, and Fisher’s test was used when χ2 conditions were not met.
RESULTS
Within the analysed six-month period, 8199 patients underwent surgery: 350 were operated on under local anaesthesia, 2050 had regional anaesthesia and 5799 received general anaesthesia (Figure 1). Data from 909 patients were taken into analysis. Patients’ demographics and surgery type distribution are shown in Table 1. Airway assessment scores and characteristics of airway management and devices used are shown in Table 2. Complications during airway management occurred in 50 patients; the distribution of complications is presented in Table 3. The most prevalent complication, found in 22 patients (2.09%), was difficult airway, defined as problems with ventilation and/or airway device placement – difficult ventilation occurred in nine cases, in seven there was difficult tracheal intubation and one patient experienced difficult SAD placement. In five patients, both difficult mask ventilation and difficult tracheal intubation occurred. There were no statistically significant differences in age and gender distribution between patients with and without any complication (P > 0.05). Body mass index (BMI) value of patients in the group with complications was found to be significantly higher compared to BMI of those in the group without complications (P = 0.013).
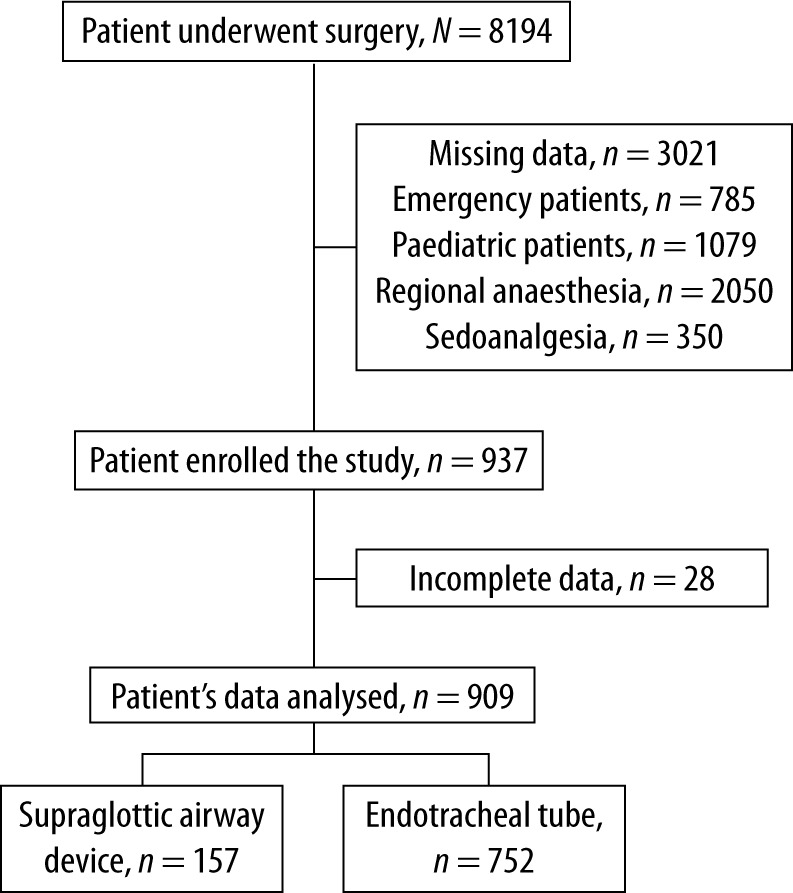
TABLE 1
Demographic data of patients, frequency of complications, range of surgery type
TABLE 2
Airway assessment scores, characteristics of airway management and devices used. Number of airway management attempts presented as minimal, maximal values and mean ± SD; other parameters as numbers and percentage
TABLE 3
Complications during airway management
Airway trauma occurred in 19 patients. In 6 patients blood was found on airway equipment: in three cases there was blood on the SAD and in three cases on the endotracheal tube. Five patients had pharynx injuries, five had lip injuries and three had teeth and lip injuries.
The Cormack-Lehane, Mallampati and ventilation score in the group of patients with complications were significantly higher compared to values found in those without complications (P < 0.05). When a Macintosh blade was used during tracheal intubation, more complications occurred compared to Miller blade use. Concerning supraglottic airway devices, there was no significant difference in complications among classical laryngeal mask airway (LMA), ProSeal LMA and LMA Supreme (P > 0.05). The complication rate was significantly lower when LMA Protector was used (Table 4).
TABLE 4
Comparison of patient data in respect of complication occurrence. Age and body mass index are presented as mean ± SD and median, the rest of data in numbers and percentage
| Parameter | Complication – no | Complication – yes | P | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD/n % | Median | Mean ± SD/n % | Median | ||||
| Age (years) | 48.0 ± 15.9 | 47.0 | 51.1 ± 15.3 | 51.5 | 0.197m | ||
| Gender | |||||||
| Male | 359 | 41.8% | 23 | 46.0% | 0.558x2 | ||
| Female | 500 | 58.2% | 27 | 54.0% | |||
| BMI (kg m−2) | 27.3 ± 5.1 | 27.0 | 29.4 ± 6.5 | 30.0 | 0.013m | ||
| Surgery | |||||||
| Abdominal | 410 | 47.7% | 30 | 60.0% | 0.091x2 | ||
| Extra-abdominal | 449 | 52.3% | 20 | 40.0% | |||
| Cormack-Lehane | |||||||
| I | 399 | 54.4% | 14 | 29.8% | 0.001x2 | ||
| II | 253 | 34.5% | 11 | 23.4% | |||
| III | 76 | 10.4% | 11 | 23.4% | |||
| IV | 6 | 0.8% | 11 | 23.4% | |||
| Mallampati | |||||||
| I | 296 | 34.5% | 9 | 18.0% | 0.017x2 | ||
| II | 501 | 58.3% | 27 | 54.0% | |||
| III | 55 | 6.4% | 13 | 26.0% | |||
| IV | 7 | 0.8% | 1 | 2.0% | |||
| Ventilation score | |||||||
| I | 651 | 75.8% | 20 | 40.0% | 0.000x2 | ||
| II | 146 | 17.0% | 10 | 20.0% | |||
| III | 58 | 6.8% | 14 | 28.0% | |||
| IV | 4 | 0.5% | 6 | 12.0% | |||
| Type of airway device | |||||||
| Tracheal tube | 704 | 82.0% | 44 | 88.0% | 0.276x2 | ||
| Classic LMA | 19 | 2.2% | 2 | 4.0% | 0.323x2 | ||
| ProSeal | 23 | 2.7% | 1 | 2.0% | 1.000x2 | ||
| Supreme | 5 | 0.6% | 2 | 4.0% | 0.052x2 | ||
| LMA Protector | 108 | 12.6% | 1 | 2.0% | 0.025x2 | ||
| Type of blade | |||||||
| Miller | 156 | 18.2% | 3 | 6.0% | 0.028x2 | ||
| Macintosh | 703 | 81.8% | 47 | 94.0% | |||
There was no significant difference in demographic data including age, gender, BMI values or Mallampati scores in patients who had 3 or more attempts for intubation. The Cormack-Lehane and ventilation scores of these patients were significantly higher (P < 0.001, P = 0.009, respectively, Table 5). While there was no significant difference in number of attempts among classic LMA, ProSeal LMA and LMA Supreme, the number of attempts significantly decreased with LMA Protector use (P = 0.003). When the Miller blade was used, no case required more than 2 attempts, while in 62 cases of Macintosh blade use, 3 or more efforts were noted (Table 5).
TABLE 5
Correlation analysis of demographic data, airway assessment scores and type of airway device in terms of number of attempts. Age and body mass index are presented as mean ± SD and median, the rest of parameters in numbers and percentage
| Parameter | Number of attempts < 3 | Number of attempts ≥ 3 | P | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD/n % | Median | Mean ± SD/n % | Median | ||||
| Age (years) | 48.2 ± 16.0 | 48.0 | 48.0 ± 14.2 | 46.5 | 0.864m | ||
| Gender | |||||||
| Male | 356 | 42.0% | 26 | 41.9% | 0.988x2 | ||
| Female | 491 | 58.0% | 36 | 58.1% | |||
| BMI (kg m−2) | 27.4 ± 5.2 | 27.0 | 28.3 ± 5.2 | 28.0 | 0.180m | ||
| Surgery | |||||||
| Abdominal | 412 | 48.6% | 28 | 45.2% | 0.597x2 | ||
| Extra-abdominal | 435 | 51.4% | 34 | 54.8% | |||
| Cormack-Lehane | |||||||
| I | 397 | 55.2% | 16 | 25.8% | 0.000x2 | ||
| II | 241 | 33.5% | 23 | 37.1% | |||
| III | 75 | 10.4% | 12 | 19.4% | |||
| IV | 6 | 0.8% | 11 | 17.7% | |||
| Mallampati | |||||||
| I | 291 | 34.4% | 14 | 22.6% | 0.058x2 | ||
| II | 496 | 58.6% | 32 | 51.6% | |||
| III | 54 | 6.4% | 14 | 22.6% | |||
| IV | 6 | 0.7% | 2 | 3.2% | |||
| Ventilation score | |||||||
| I | 634 | 74.9% | 37 | 59.7% | 0.009x2 | ||
| II | 142 | 16.8% | 14 | 22.6% | |||
| III | 63 | 7.4% | 9 | 14.5% | |||
| IV | 8 | 0.9% | 2 | 3.2% | |||
| Type of airway device | |||||||
| Tracheal tube | 686 | 81.0% | 62 | 100% | 0.000x2 | ||
| Classic LMA | 21 | 2.5% | 0 | 0.0% | 0.390x2 | ||
| ProSeal | 24 | 2.8% | 0 | 0.0% | 0.401x2 | ||
| Supreme | 7 | 0.8% | 0 | 0.0% | 1.000x2 | ||
| LMA Protector | 109 | 12.9% | 0 | 0.0% | 0.003x2 | ||
| Blade type | |||||||
| Miller | 159 | 18.8% | 0 | 0.0% | 0.000x2 | ||
| Macintosh | 688 | 81.2% | 62 | 100% | |||
There was no significant difference in demographic parameters such as age, gender or BMI values in patients with rescue airway devices use compared to those who did not require such device, while Cormack-Lehane, Mallampati and ventilation scores were significantly higher (P = 0.029, P = 0.002, P = 0.026, respectively) (Table 6). When rescue airway devices were used, no significant difference was observed compared to SAD or blade type.
TABLE 6
Correlation analysis of demographic data, airway assessment scores and airway devices in terms of the need for rescue technique. Age and body mass index are presented as mean ± SD and median, the rest of parameters in numbers and percentage
| Parameter | Rescue technique – no | Rescue technique – yes | P | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD/n % | Median | Mean ± SD/n % | Median | ||||
| Age (years) | 48.0 ± 15.9 | 47.0 | 54.4 ± 15.9 | 52.5 | 0.095m | ||
| Gender | |||||||
| Male | 372 | 42.0% | 10 | 41.7% | 0.971x2 | ||
| Female | 513 | 58.0% | 14 | 58.3% | |||
| BMI (kg m−2) | 27.4 ± 5.2 | 27.0 | 29.1 ± 5.4 | 29.0 | 0.137m | ||
| Surgery | |||||||
| Abdominal | 426 | 48.1% | 14 | 58.3% | 0.324x2 | ||
| Extra-abdominal | 459 | 51.9% | 10 | 41.7% | |||
| Cormack-Lehane | |||||||
| I | 406 | 53.6% | 7 | 30.4% | 0.029x2 | ||
| II | 262 | 34.6% | 2 | 8.7% | |||
| III | 83 | 10.9% | 4 | 17.4% | |||
| IV | 7 | 0.9% | 10 | 43.5% | |||
| Mallampati | |||||||
| I | 304 | 34.4% | 1 | 4.2% | 0.002x2 | ||
| II | 513 | 58.0% | 15 | 62.5% | |||
| III | 62 | 7.0% | 6 | 25.0% | |||
| IV | 6 | 0.7% | 2 | 8.3% | |||
| Ventilation score | |||||||
| I | 658 | 74.4% | 13 | 54.2% | 0.026x2 | ||
| II | 149 | 16.8% | 7 | 29.2% | |||
| III | 69 | 7.8% | 3 | 12.5% | |||
| IV | 9 | 1.0% | 1 | 4.2% | |||
| Type of airway device | |||||||
| Tracheal tube | 726 | 82.0% | 22 | 91.7% | 0.223x2 | ||
| Classic LMA | 20 | 2.3% | 1 | 4.2% | 0.433x2 | ||
| ProSeal | 23 | 2.6% | 1 | 4.2% | 0.478x2 | ||
| Supreme | 7 | 0.8% | 0 | 0.0% | 1.000x2 | ||
| LMA Protector | 109 | 12.3% | 0 | 0.0% | 0.068x2 | ||
| Type of blade | |||||||
| Miller | 157 | 17.7% | 2 | 8.3% | 0.231x2 | ||
| Macintosh | 728 | 82.3% | 22 | 91.7% | |||
A stylet was used more frequently in patients anesthetised for abdominal surgery compared to non-abdominal (P < 0.001) (Table 7). There was no significant difference in the demographic parameters such as age, gender or BMI values between patients intubated using a stylet compared to the non-stylet intubation group. In patients for whom a stylet was used, the Cormack-Lehane scores were significantly higher (P = 0.012); however, there was no significant difference for Mallampati or ventilation scores. When compared to the Miller blade, the use of a Macintosh blade required a higher stylet ratio (P < 0.001).
TABLE 7
Correlation analysis among demographic data, airway assessment scores and airway devices in terms of the need for stylet use. Age and body mass index are presented as mean ± SD and median, the rest of parameters in numbers and percentage
| Parameter | Stylet (−) | Stylet (+) | P | ||||
|---|---|---|---|---|---|---|---|
| Mean±SD/n-% | Median | Mean±SD/n-% | Median | ||||
| Age (years) | 48.9 ± 16.1 | 48.0 | 46.9 ± 15.3 | 46.0 | 0.099m | ||
| Gender | |||||||
| Male | 244 | 40.2% | 138 | 45.7% | 0.114x2 | ||
| Female | 363 | 59.8% | 164 | 54.3% | |||
| BMI (kg m−2) | 27.4 ± 5.1 | 27.0 | 27.6 ± 5.3 | 27.0 | 0.410m | ||
| Surgery | |||||||
| Abdominal | 226 | 37.2% | 214 | 70.9% | 0.000x2 | ||
| Extra-abdominal | 381 | 62.8% | 88 | 29.1% | |||
| Cormack-Lehane | |||||||
| I | 261 | 54.5% | 152 | 50.3% | 0.012x2 | ||
| II | 162 | 33.8% | 102 | 33.8% | |||
| III | 52 | 10.9% | 35 | 11.6% | |||
| IV | 4 | 0.8% | 13 | 4.3% | |||
| Mallampati | |||||||
| I | 211 | 34.8% | 94 | 31.1% | 0.141x2 | ||
| II | 354 | 58.3% | 174 | 57.6% | |||
| III | 38 | 6.3% | 30 | 9.9% | |||
| IV | 4 | 0.7% | 4 | 1.3% | |||
| Ventilation score | |||||||
| I | 446 | 73.5% | 225 | 74.5% | 0.654x2 | ||
| II | 106 | 17.5% | 50 | 16.6% | |||
| III | 50 | 8.2% | 22 | 7.3% | |||
| IV | 5 | 0.8% | 5 | 1.7% | |||
| Type of airway device | |||||||
| Tracheal tube | 73.85 | 73.8% | 300 | 99.3% | 0.000x2 | ||
| Classic LMA | 20 | 3.3% | 1 | 0.3% | 0.005x2 | ||
| ProSeal | 24 | 4.0% | 0 | 0.0% | 0.000x2 | ||
| Supreme | 7 | 1.2% | 0 | 0.0% | 0.061x2 | ||
| LMA Protector | 108 | 17.8% | 1 | 0.3% | 0.000x2 | ||
| Type of blade | |||||||
| Miller | 157 | 25.9% | 2 | 0.7% | 0.000x2 | ||
| Macintosh | 450 | 74.1% | 300 | 99.3% | |||
DISCUSSION
In this six-month observational study, conducted in a university hospital, aimed at analysis of airway complications that occurred during general anaesthesia induction, complication prevalence was 5%. The three most common problems were difficult airway, hypoxemia and airway trauma. Mild and moderate complications were the most common and severe airway complications were not observed.
Fifty patients (5%) developed complications. Although a six-month period was analysed, emergency patients were not included in this study. This allowed the monitoring of patients over a 130-business day frame, during which it was revealed that an airway-related complication occurred every 2.5 days. This result shows that airway complications are frequent and should not be overlooked. Additionally, it has been revealed that the concept that airway complication development prevalence is relatively low is not the case.
According to data from 114,904 patients, analysed in the NAP4 study, 184 serious airway complications were reported [2]. Thirty-three patients died due to airway problems: 14 of them died during anaesthesia, 16 died in the ICU and 3 died in the emergency department. Brain damage occurred in 3 patients during anaesthesia. Additionally, the NAP4 reported that emergency surgical airway interventions were performed in 58 cases with anaesthesiologists as the providers in 25 cases. They succeeded in 9 cases, while there were 11 failures which were rescued by a surgeon-performed tracheostomy. One patient died and three patients were intubated.
In contrast, in our study, there were no deaths reported, and no one required surgical airway intervention or admission to the Intensive Care Unit due to airway-related complications. We believe that this result is attributable to the monocentre structure of this study.
The most common problem in patients with difficult airways was difficult mask ventilation, followed by difficult tracheal intubation. Similarly, in a closed case analysis in England, inadequate ventilation accounted for 12.7% of all airway-related claims [8]. A meta-analysis that investigated complications during and after general anaesthesia from 10 randomised controlled studies reported difficult tracheal intubation in more than half of those studies [9]. In our study, in more than 50% of the difficult ventilation cases, problems occurred also during tracheal intubation. This result contradicts another result in the NAP4 study. The most common primary airway problems in the NAP4 were tracheal intubation difficulties including difficult or delayed intubation, failed intubation, and the ‘can’t intubate can’t ventilate’ situation. This result was not surprising because it is reported that difficult mask ventilation prevalence ranges from 0.08 to 15% [10].
According to the American Society of Anesthesiologists Closed Claims Project Database, an airway injury was reported in 6% of 4,460 claims [11]. In our study, airway trauma occurred in 19 patients. In most of these cases, blood on the tracheal tube was observed when the laryngeal mask was removed or the patient was intubated. However, since no active bleeding or deep injury was observed during mouth examination, these were recorded as mild complications.
While age and gender showed no significant effect on airway complication occurrence, it was found that BMI value was an independent predictor of complications. In our study, it was found that high scores in the Cormack-Lehane and Mallampati tests that are commonly used in clinical practice cannot predict various difficulties with airway management. The Cormack-Lehane, Mallampati and ventilation scores in patients with complications were significantly higher than in the group of patients without complications. The Cormack-Lehane and ventilation scores were predictors for multiple intervention numbers. However, demographic parameters such as age, gender, BMI value and Mallampati score were shown not to be predictive of a high intervention number. A high percentage of false-positive results indicated in previous studies for Mallampati tests was supported by our study [12]. Similarly, a review by Cochrane identified Mallampati sensitivity as 0.53 and specificity as 0.80 [13]. In our study, the Cormack-Lehane, Mallampati and ventilation scores were indicators for rescue airway requirements. However, in terms of the need for the use of a stylet, only the Cormack-Lehane score had predictive value.
The LMA Protector is a new SAD that has been implemented in clinical practice in recent years [14]. A significant decrease of complications has been found when the LMA Protector was used, but at the same time, the number of interventions with the LMA Protector has been significantly lower. Previous studies on the LMA Protector are controversial. While one preliminary study concluded that the device provided a fast insertion time and a reliable and adequate airway seal, a recent study showed that compared to problems that emerge with a traditional laryngeal mask such as reposition rates and hemodynamic disturbances, LMA Protector use revealed no significant differences [15, 16].
Huitink et al. [6] determined the complication rates in their institution; however, these data were collected as self-reports through interviews. Voluntary reporting of complications may not be reliable and may miss several events. In our study researchers were not a part of operating theatre staff anaesthesiologists involved in the anaesthesia of analysed cases and data recording and analysis were completed on an unequivocal observational basis. The results of this study raise awareness concerning minor or major complications that occur in daily anaesthesia practice. We believe that this knowledge contributes to increasing patient safety.
LIMITATIONS
One of the limitations of this study is that not all patients operated on under general anaesthesia during the six-month period were included in the analysis. A lack of manpower and patient caseloads are the main reasons for this limitation. Therefore, data for paediatric patients were not recorded. Another limitation was exclusion of emergency patients since it is known that complication risks increase during emergency airway management. It is believed that future studies, which will include those missed groups, will be planned.
CONCLUSIONS
The prevalence of airway-related complications during anaesthesia induction and maintenance of anaesthesia was not low; the most common complication was difficult mask ventilation. We concluded that a preoperative assessment test was insufficient to predict the problems. Moreover, it was found that hypoxemia was a common cause among preventable complications.