





The haemodynamically effective heart function largely depends on the normal diastolic function of its muscle. The correct filling of the left ventricle and its ejection volume, secondary to it, depend on myocardial diastolic performance [1]. The left ventricular diastolic function is significantly affected by hemodynamic conditions, i.e. the heart rate and the left ventricular filling time associated with it, preload, and afterload, although to a lesser extent. Transient or permanent disturbances of left ventricular diastole can lead to an increase in its lumen pressure and impairment of the blood inflow from the left atrium and the pulmonary circulation [2].
The evaluation of diastolic function is not only of great importance for the diagnosis of heart failure, primarily with preserved left ventricular ejection fraction (HFpEF) [1], but also for the assessment of the hemodynamic state of a patient with acute heart failure (AHF). A detailed algorithm for HFpEF recognition was suggested in the recently developed guidelines of the Association of Heart Failure of the European Society of Cardiology [3]. It should, however, be emphasized that the term HFpEF refers to a clinical diagnosis involving a much broader spectrum of patients than just patients with left ventricular diastolic disorders, whose presence is not a necessary condition for the diagnosis of HFpEF. For obvious reasons, the diastolic exercise test used in patients with suspected HFpEF has a limited application in the context of patients hospitalized in intensive care units. Correct estimation of the left ventricular filling pressures may be crucial, especially in AHF patients. Echocardiographic examinations enable non-invasive bedside assessment of these pressures [2] and understanding the pathophysiology and hemodynamic consequences of diastolic dysfunction facilitates accurate clinical decisions.
Although precise assessment of the left ventricular diastolic function is beyond the scope of the point-of-care examination, knowing the basics of physiology it is not difficult to learn how to record basic echocardiographic parameters describing left ventricular diastole and how to interpret them. At the same time, such abilities are very useful in routine work in the intensive care unit and during anaesthesia. The following text is intended to familiarize the reader with the basics of left ventricular diastolic function assessment and to present the most important information regarding its significance.
BASICS OF ECHOCARDIOGRAPHIC ASSESSMENT OF LEFT VENTRICULAR DIASTOLIC FUNCTION
Trying to assess the left ventricular diastolic function, we ask ourselves questions about the degree of active relaxation dysfunction (a process that requires energy expenditure), about passive left ventricular compliance (determined by structural changes in the muscle), and preload (secondary to hemodynamic conditions). Disorders of these three elements are crucial for left ventricular dysfunction during diastole.
In order to initially assess the left ventricular diastolic function, the answers to the following questions should be useful: (1) How does the left ventricle fill? (2) How does the muscle deform in diastole? (3) Does this lead to an increase in left ventricular filling pressure? and (4) Does this lead to left atrial enlargement/remodelling?
Several measurement methods are used in echocardiographic assessment of the left ventricular diastolic function.
(1) When assessing left ventricular filling, we use the mitral inflow profile in the pulsed wave (PW) Doppler ultrasound examination (Figure 1). The E wave corresponds to the early blood flow from the left atrium to the left ventricle, while the A wave results from the contraction of the left atrium.
FIGURE 1
Assessment of mitral inflow in pulsed wave (PW) examination. In the diastolic phase, blood flows from the left atrium to the left ventricle through the open mitral valve. In cases of sinus rhythm and effective contraction of the left atrium, the inflow is of a two-phase nature. The first early wave (E wave) is associated with the pressure difference between the atrium and the ventricle, and the second wave (A [atrium] wave) – with atrial contraction and pushing of additional blood volume in its final phase

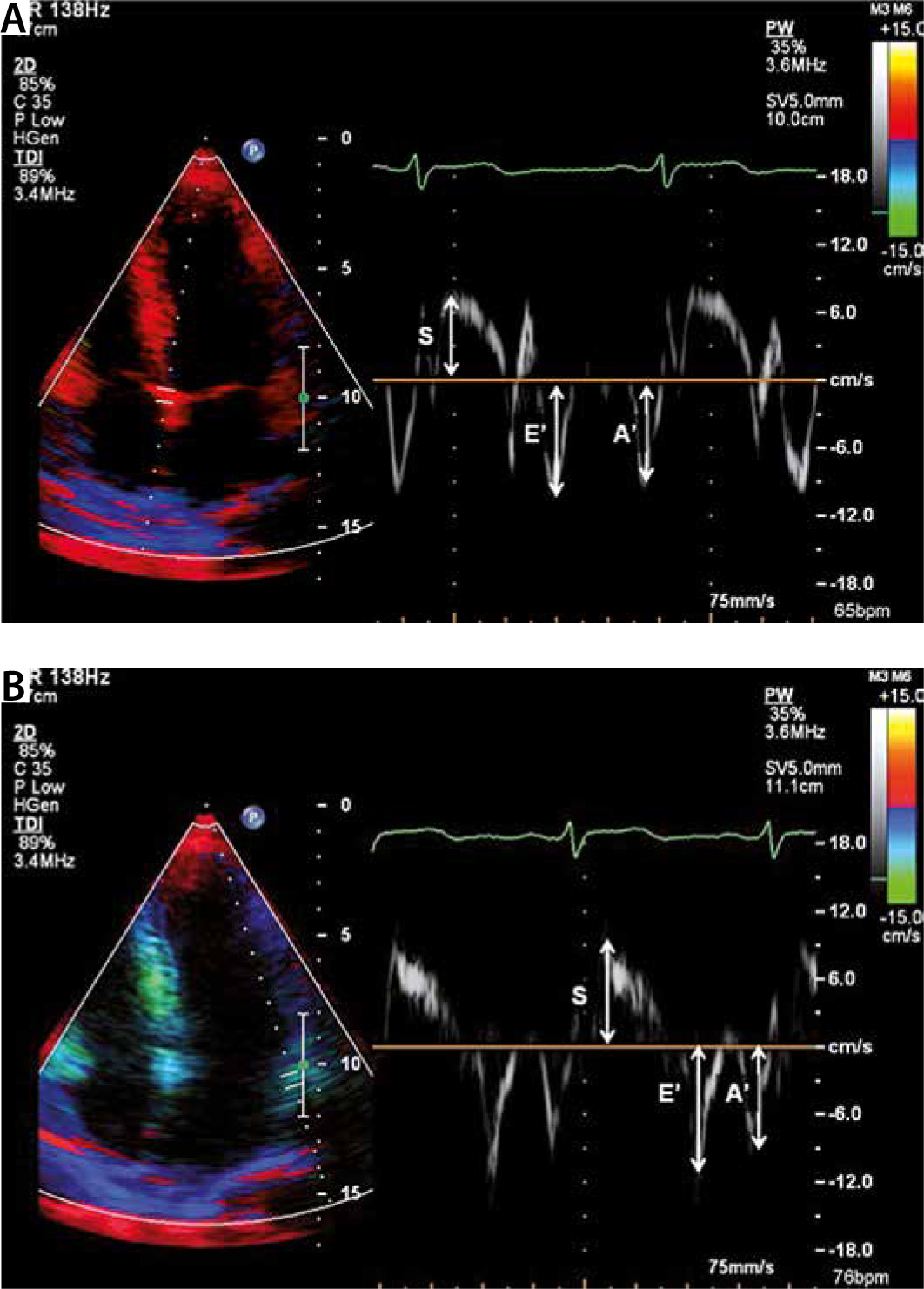
(2) Tissue Doppler imaging (TDI) is used to assess left ventricular muscle deformation. The S wave results from the movement of the mitral ring during left ventricular contraction, while e’ and a’ waves correspond to muscle movement caused by the inflow of blood from the left atrium to the left ventricle during early inflow (e’) and atrial contraction (a’) (Figure 2) [3].
FIGURE 2
Evaluation of left ventricular muscle deformation in a tissue Doppler echocardiography. In the tissue Doppler imaging study, the record of muscle movement speed (and not of blood, as in the classic Doppler!) reflects the movement of the medial and lateral parts of the mitral ring during the diastole. The higher the muscle speed (e’), the better the preserved left ventricular diastolic function


Increased left ventricular filling pressures are estimated by means of a derivative parameter of the previous two, i.e. E/e’ (Figure 3), correlating well with the end-diastolic pressure in the left atrium and the reverse gradient through the tricuspid valve, correlating well with the systolic pressure in the pulmonary artery (Figure 4).
FIGURE 3
Left ventricular filling pressure assessment, E/e’ parameter. E/e’ – the ratio of the early influx wave (E) velocity and the corresponding velocity of the left ventricular muscle (measured in the medial or lateral part of the mitral ring) (e’). E/e’ parameter best correlates with left ventricular filling pressures. Values greater than 14, as in this case, correspond to the increased filling pressure of the left ventricle
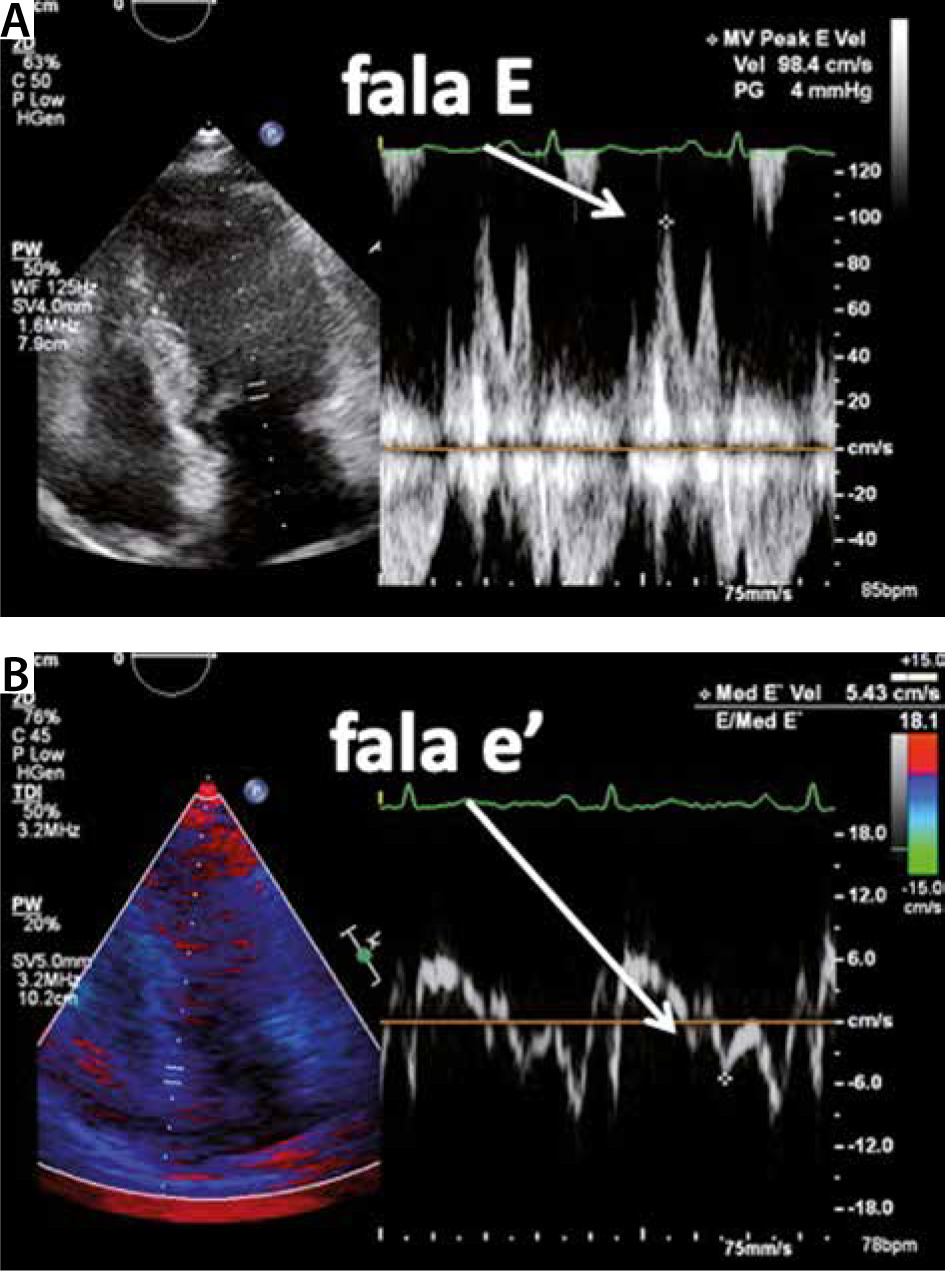
FIGURE 4
Left ventricular filling pressure assessment, reverse gradient through a tricuspid valve. The maximum tricuspid regurgitation velocity (TRV) determined in a continuous Doppler, e.g. in a four-chamber projection, correlates with the systolic pressure in the pulmonary artery. TRV values less than 2.8 m s−1 indicate a low probability of pulmonary hypertension

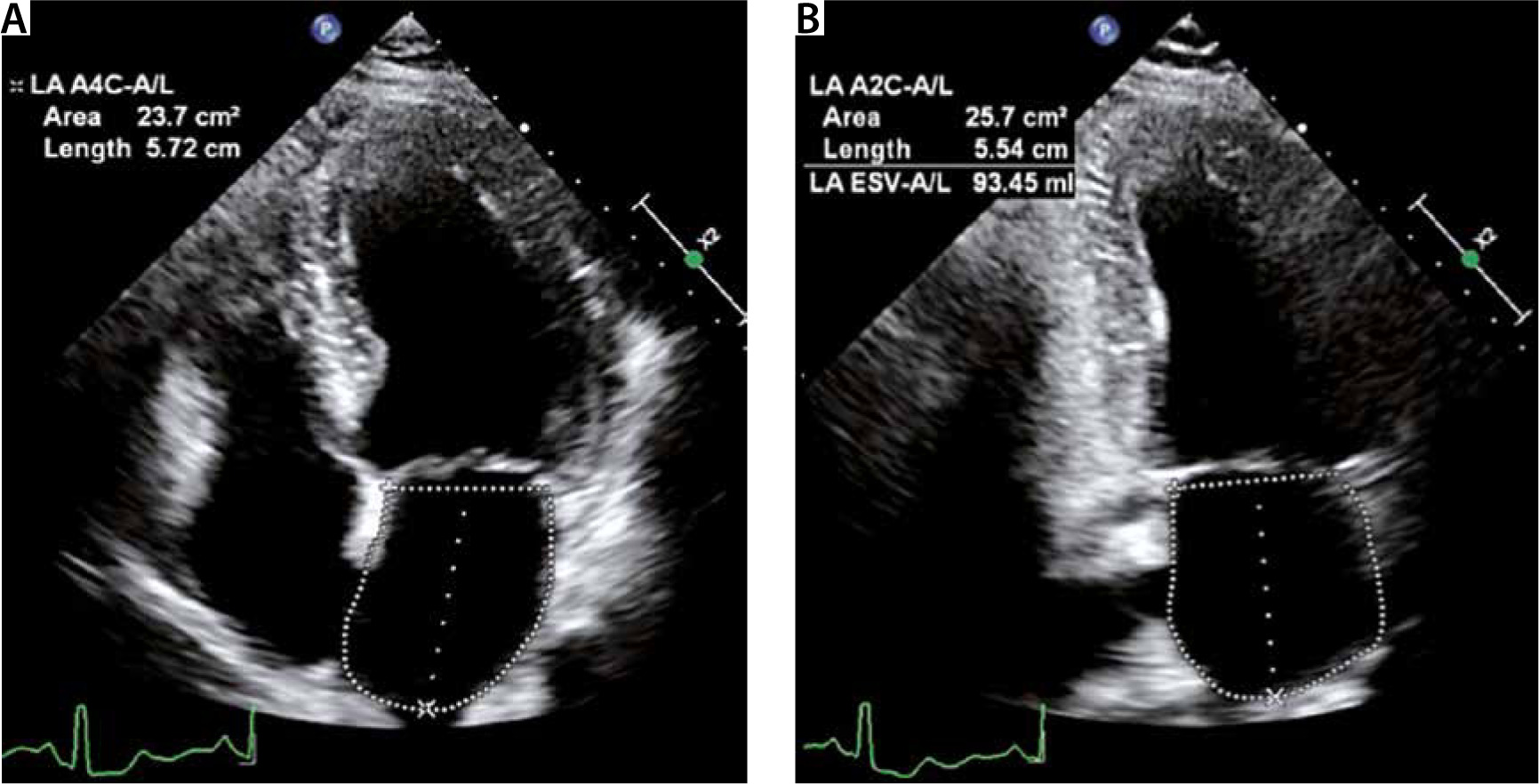
The left atrium enlargement is evaluated by measuring its size and volume (Figure 5).
FIGURE 5
Assessment of the dimensions and volume of the left atrium. Remodelling, or increased volume, of the left atrium is the consequence of diastolic dysfunction and increased pressures therein. We consider it significant if the left atrium surface area in the four-chamber apical projection exceeds 20 cm2 and the volume indexed to the body surface is greater than 34 mL m−2. Most modern cameras measure the volume of the left atrium automatically, basing on three measurements: surface area in a four-chamber projection, surface area in a dual-chamber projection and the upper-lower dimension. The volume is calculated according to the formula:
where A1 is the atrium area in the four-chamber projection, A2 – in the dual chamber projection and L – the upper-lower dimension of the atrium
LA – left atrium, LAVI – left atrial volume index, BSA – body surface area
A DIAGNOSTIC ALGORHITHM OF DIASTOLIC DYSFUNCTION IN PATIENTS WITH NORMAL LEFT VENTRICULAR EJECTION FRACTION
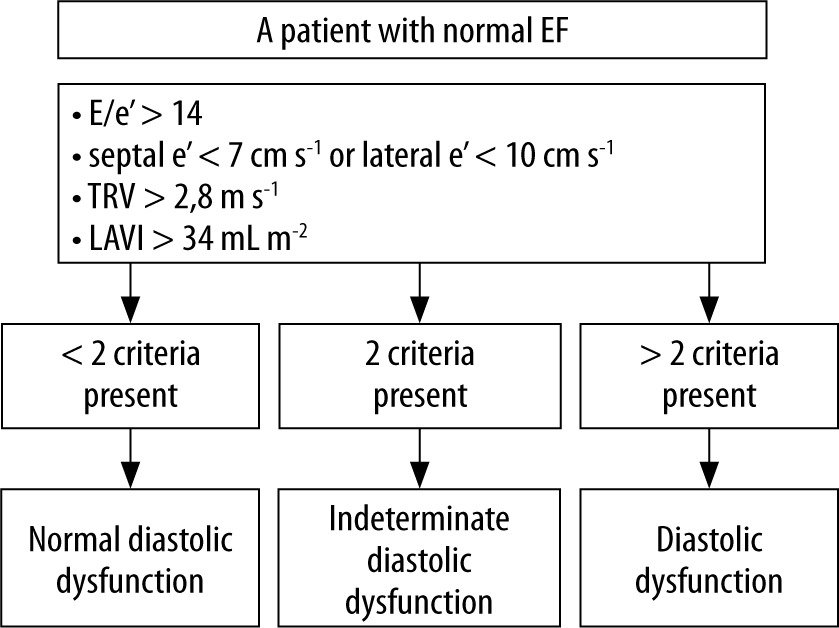
In the case of normal left ventricular ejection fraction values, the diagnosis of diastolic dysfunction is based on a systematic assessment of four parameters (Figure 6). Such an algorithm has been proposed in the current guidelines [2]. Below the reader will find a more detailed discussion of this algorithm. The evaluated parameters are: (1) E/e’ ratio (the higher, the more likely diastolic dysfunction), (2) e’ wave – velocity of the mitral ring measured in the septum area or laterally (the lower the velocity values in diastole, the greater the diastolic dysfunction), (3) maximum tricuspid regurgitation velocity (TRV) (the higher the speed, the greater the systolic pressure in the pulmonary artery, as a result of diastolic dysfunction), (4) the left atrial volume index (LAVI) (a large left atrium may indirectly mean increased left ventricular filling pressure). The way in which we determine the values of the above four parameters is discussed and presented in Figures 1–5. Moreover, Figure 6 shows the cut-off points of these values used in this algorithm. Their assessment is included in the standard echocardiography protocol performed on a device with the tissue Doppler option, i.e. on most modern devices with a cardiological option currently available on the market. The presence of three or four abnormal values enables the diagnosis of diastolic dysfunction, while less than two abnormalities lead to the diagnosis of normal diastolic function. In clinical practice, we often find only two incorrect values, e.g. the left atrium is enlarged and the mitral ring speed is slightly reduced, but there is no increase in the velocity of retrograde tricuspid regurgitation, or in the E/e’ ratio. Another, not infrequent, situation is tricuspid regurgitation with an increased rate of retrograde wave and left atrial enlargement. In such a situation, the diastolic function assessment should be extended by a precise assessment of the left ventricular filling profile, and sometimes also by other parameters, such as assessment of pulmonary vein flow, mitral inflow propagation rate and others. In simple terms, it can be assumed that the ratio of the left ventricular filling waves during diastole will change depending on the increase in pressure in the left atrium, and the time of early filling will increase with progressive disorders of the left ventricle relaxation. An analysis of the E and A wave ratio and deceleration time allows to determine the degree of diastolic dysfunction. It is very helpful, especially in patients with reduced left ventricular ejection fraction, to record the blood inflow from the pulmonary veins to the left atrium. The change in the inflow ratio during the systole and diastole (S and D waves, respectively) correlates with the left ventricular filling pressures [2]. However, as the authors emphasize, such an assessment is often infeasible in the intensive care unit.
FIGURE 6
Diagnostic algorithm of diastolic dysfunction in patients with normal left ventricular ejection fraction. The above algorithm is discussed in the text
TRV – tricuspid regurgitation velocity, LAVI – left atrial volume index, E/e’ – the ratio of the velocity of the early influx wave (E) to the corresponding velocity of the left ventricular muscle (measured in the medial or lateral part of the mitral ring) (e’)
SIMPLIFIED ASSESSMENT OF LEFT VENTRICULAR DIASTOLIC FUNCTION
In accordance with the guidelines of the American Echocardiographic Society, assessment of the diastolic function goes beyond the point-of-care bedside examination. An evaluation of the four required parameters may be impossible for technical reasons (e.g. worse imaging conditions in mechanically ventilated patients) or too time-consuming to be adapted for the needs of intensive care. The article published in the Critical Ultrasound Journal suggested a simplified examination of left ventricular diastolic dysfunction, limited only to assessing the velocity of the septum and sidewall e’ waves [4]. Diastolic dysfunction was identified as average e’ wave measurements from the septum and sidewall. The cut-off point was < 9 cm s−1 as the only parameter evaluated. The examination was performed by emergency medicine doctors, who had limited experience in performing echocardiography. Subsequently, the patients identified in this way were subjected to an echocardiographic examination performed by a cardiologist according to the current guidelines for diastolic dysfunction assessment. Diastolic dysfunction was confirmed in 41 out of 48 patients and the kappa ratio was 0.74 (95% CI: 0.57–0.92). However, such simplification is at high risk of making a mistake, especially in situations where a change in the mobility of the mitral ring may not be due to changes in the diastolic function (e.g. advanced systolic heart failure, atrial fibrillation, ventricular dyssynchronism, or regional contractility disorders) [5–7]. The American Echocardiographic Society states in its guidelines that, due to the numerous hemodynamic variables that may affect the assessed parameters, no parameter should be taken into account individually when assessing diastolic function. Therefore, the clinical context is extremely important for the point-of-care examination. If the E/e’ index exceeds 15 on the bedside examination and the lung ultrasound shows features of pulmonary oedema, heart failure can be recognised with 100% sensitivity and 95.8% specificity [8].
LEFT VENTRICULAR DIASTOLIC DYSFUNCTION – SIGNIFICANCE FOR AN ANAESTHESIOLOGIST
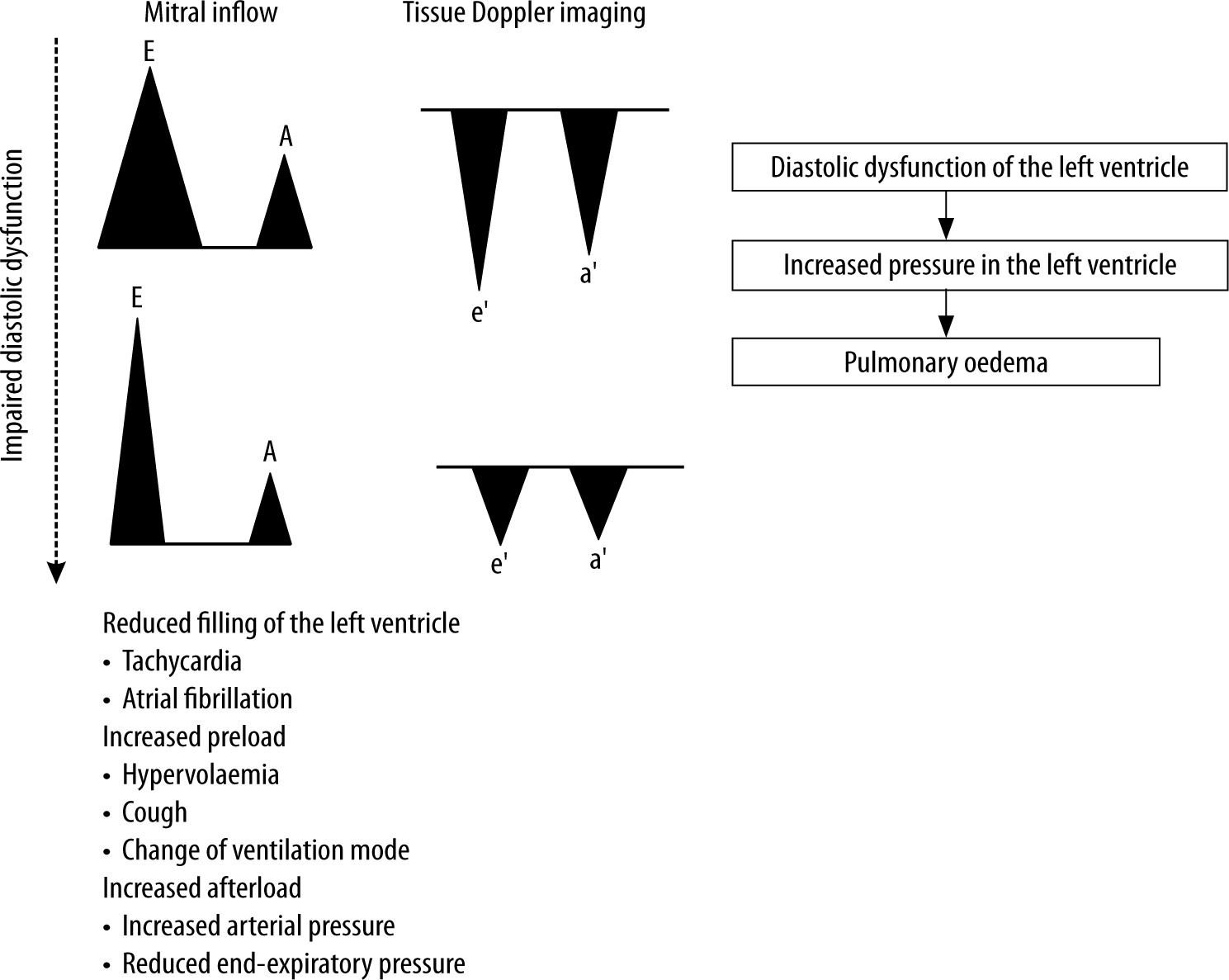
The prevalence of diastolic dysfunction among individuals over 60 years is estimated at 28% [9]. Patients with diastolic dysfunction are less able to compensate for changes in vascular bed filling or for cardiac arrhythmias that may occur during surgery. Increased left ventricular filling pressure in hypervolemia can lead to pulmonary oedema, while in hypovolemia it can significantly reduce cardiac output. The hemodynamic stability of a patient with diastolic dysfunction depends on the heart rhythm and the effectiveness of the left atrial contraction, which affect the time of left ventricular diastole and the volume of its filling prior to contraction (Figure 7).
FIGURE 7
Mechanisms leading to exacerbation of diastolic heart failure. Exacerbation of diastolic heart failure may occur as a result of hemodynamic changes in the patient, e.g. during removal of the endotracheal tube (stimulation of the sympathetic nervous system, cough reflex, change in end-expiratory pressure). As a result of deterioration of left ventricular muscle compliance, pressure in the left atrium increases, which can result in pulmonary oedema
The presence of left ventricular diastolic dysfunction is an independent factor in 30-day mortality in patients undergoing surgery [10]. Nevertheless, it has not been included in the commonly used perioperative risk assessment scales. Therefore, it can be assumed that the risk of complications in patients with impaired diastolic function is underestimated.
RISK FACTORS FOR LEFT VENTRICULAR DIASTOLIC DYSFUNCTION (TABLE 1) [3]
TABLE 1
Risk factors for left ventricular diastolic dysfunction
| Age |
| Being female |
| Hypertension |
| Ischaemic heart disease |
| Diabetes |
| Kidney failure |
| Obesity |
| Anaemia |
| Chronic obstructive pulmonary disease |
| Obstructive sleep apnoea |
For anaesthetists, information about diastolic dysfunction may be as important as information about myocardial systolic dysfunction or the presence of valvular disease. Identification of patients with left ventricular diastolic dysfunction may have a significant impact on the perioperative period because limited myocardial compliance may require appropriate monitoring and individual therapeutic approach in terms of fluid therapy as well as drugs modifying the cardiac function.
PERIOPERATIVE MANAGEMENT
Patients with left ventricular diastolic dysfunction have limited capacity to compensate for cardiac output in response to haemodynamic changes that may occur during surgery. The tolerance range for fluid supply in this group of patients is very limited [11]. The time of induction of general anaesthesia is therefore critical, as hypotension often occurs due to dilatation of the vascular bed and reduction of venous flow. Excessive fluid therapy may be equally dangerous, leading to a sharp increase in left ventricular filling pressure and pulmonary oedema [12].
In people with left ventricular diastolic dysfunction, the occurrence of cardiac arrhythmias or tachycardia may lead to a sharp decrease in cardiac output due to a decrease in left ventricular filling [13]. The anaesthetist should make every effort to avoid excessive adrenergic stimulation during intubation and removal of the endotracheal tube.
Therefore, it is recommended that people with left ventricular diastolic dysfunction be considered as patients at high risk for perioperative cardiovascular complications. Such information should also be provided to the patient during the preoperative anaesthetic visit. In the context of an increased risk of perioperative hemodynamic instability, consideration should be given to extending the scope of cardiovascular function monitoring and prior preparation of a pressor amine solution [11].
DIASTOLIC DYSFUNCTION AND PERIOPERATIVE COMPLICATIONS IN CARDIAC SURGERY
In patients undergoing coronary artery bypass surgery, the presence of diastolic dysfunction is associated with a higher incidence of major adverse cardiac events (MACE) [12]. In this group of patients, the occurrence of diastolic dysfunction increases the likelihood of using inotropic and vasoactive drugs four times [14]. In the event of difficulties in terminating extracorporeal circulation, it may be justified to use milrinone [12, 15].
DIASTOLIC DYSFUNCTION AND PERIOPERATIVE COMPLICATIONS
Numerous studies presented in systematic reviews and meta-analyses show that the presence of left ventricular diastolic dysfunction is an independent risk factor for cardiovascular complications in the perioperative period [16–20].
The echocardiographic study conducted in 1005 patients before vascular surgery procedures demonstrated that diastolic dysfunction was present in 50% of study patients, 80% of which were asymptomatic; moreover, diastolic dysfunction was found to be a risk factor for cardiovascular complications within the 30 postoperative period [21].
In patients with a high E/e’ ratio (high left ventricular filling pressure) undergoing low and moderate risk non-cardiac surgery, the E/e’ value was a predictive factor of perioperative pulmonary oedema [22].
Furthermore, according to the data reported, the patients from this group undergoing vascular and abdominal procedures were hospitalized for a longer period [19, 23]. A study conducted in a group of 325 patients undergoing vascular procedures showed a longer hospitalization time in patients with diastolic dysfunction (7 days [5–10 days] vs. 5 days [4–6 days]; P < 0.001) [24].
An increased number of myocardial infarctions have been observed in patients with diastolic dysfunction, both in the early postoperative period (up to 48 hours) and in distant follow-up (30 days after surgery) [24, 25].
Perioperative factors exacerbating diastolic heart failure and the recommendations proposed by the authors of this study are presented in Table 2.
TABLE 2
Summary: perioperative factors exacerbating diastolic heart failure and management
WEANING OFF THE VENTILATOR
The occurrence of left ventricular diastolic dysfunction in mechanically ventilated patients is an independent risk factor for failure of weaning off the ventilator and completion of the spontaneous breathing trial (SBT) [26, 27]. The conversion of ventilation with positive airway pressures to spontaneous breathing reduces the pressure inside the chest and, consequently, increases the venous flow and adrenergic stimulation. In people with impaired left ventricular diastolic function, cardiovascular decompensation may increase under such circumstances. Increasing the preload and afterload leads to a decrease in left ventricular compliance and myocardial ischaemia, defined as weaning-induced myocardial ischaemia, or to right ventricular failure [28, 29]. Currently, there are no recommendations based on randomized studies that would indicate what kind of management strategy should be adopted in this group of patients during weaning off the ventilator and removal of the endotracheal tube. Considering pathophysiology, a reasonable strategy would be: (1) to avoid excessive adrenergic stimulation by optimizing beta-blocking therapy and ensuring adequate sedation and analgesia, (2) to reduce afterload by using diuretics [30], (3) to use positive end-expiratory pressure in the period after removal of the artificial airway [31], (4) to consider the inclusion of nitroglycerine during these activities [32], (5) to optimise the treatment of underlying diseases (hypertension, arrhythmia, asthma and chronic obstructive pulmonary disease) before removing the endotracheal tube.
SEPTIC SHOCK
Twenty-three studies carried out by Sanfilippo et al. [33], evaluating hemodynamic changes in septic shock, show that diastolic dysfunction occurred in more than 50% of cases. Left ventricular diastolic dysfunction was also an independent risk factor for mortality (no similar relationship was observed for systolic function). The authors have suggested that in the population of patients in septic shock, the parameters measured using the tissue Doppler method – e ‘wave speed and the E/e’ ratio – correlate well with diastolic dysfunction, as a parameter less susceptible to changes in preload [34]. Moreover, the e’ and E/e’ values have been found useful in fluid therapy [35]. In the ESMOSEPSIS study published in JAMA 2013, septic shock patients were randomized to treatment with an beta-adrenoceptor antagonist – esmolol, or placebo [36]. Increased cardiac output, reduced demands for noradrenaline and reduced mortality were observed in the group of patients receiving esmolol. Paradoxically, the drug which has an inotropic negative effect improved cardiac output (likely in the mechanism of slowing the heart rhythm) and thus, by improving diastolic function, improved left ventricular filling. A major limitation of the study is the fact that a mortality rate in the control group was 80%. It is possible that patients with less severe septic shock would not show such results.
CONCLUSIONS
Left ventricular diastolic dysfunction is common in patients aged > 60 years and is more frequently observed in patients undergoing vascular surgery. It is an independent risk factor for cardiovascular complications and increased mortality in the perioperative period. Patients with left ventricular diastolic dysfunction poorly tolerate tachycardia incidents, increased vascular resistance and significant fluctuations in volemia. Thanks to earlier identification of patients with diastolic dysfunction, anaesthesiologists should be able to prepare appropriately, to select suitable medications, and to decide upon the scope of vital sign monitoring. Although the study of diastolic function goes beyond the basic point-of-care examination, the ability to assess the diastolic function can be extremely useful for anaesthetists working in the operating room and in the intensive care unit.