





Dear Editor,
Ankylosing spondylitis (AS) is a chro-nic inflammatory disease, which causes inflammation and structural damage to the sacroiliac joints and spine, resulting from autoimmunity and calcium deposition. The major clinical manifestation of the early phases of AS patients are sacroiliitis, spondylitis, spondylodiscitis, and spondylarthritis. In the late phase, AS patients develop a progressive rigidity of the entire spine and sacroiliac joints and subsequent structural changes with a downward and forward shift in the spine, which leads to fixed thoracolumbar kyphosis [1, 2].
Anaesthesia management for patients with severe AS is a specific challenge to the anaesthesiologist. The limitation of cervical spine mobility and possible temporomandibular joint disease raise the potential difficulty in airway management for general anaesthesia with endotracheal intubation. In the meantime, the thoracic cage deformity causes a decrease in chest wall compliance, functional residual capacity, inspiratory capacity, and vital capacity. There is a significant increase in ventilation-perfusion mismatch, which leads to arterial hypoxemia. In the cardiovascular system, the increased pulmonary vascular resistance may lead to right ventricular hypertrophy and right heart failure. This, along with the difficulty in airway management and restrictive lung disease, increases the risk associated with general anaesthesia. At the same time, central neuraxial blocks are met with technical difficulties as a consequence of ossification of the ligament and deformity of the lumbar spine in higher grades of ankylosing spondylitis [3, 4].
We report a challenging case of a 73-year-old male with severe kyphoscoliosis, presenting with benign prostatic hyperplasia planned for transurethral resection of prostate (TURP) under regional anaesthesia. However, due to the failure of epidural anaesthesia, a scenario of esketamine combined with sevoflurane anaesthesia was successfully applied for transurethral resection of the prostate. Esketamine, a new intravenous anaesthetic with sedative and analgesic effects, was chosen because of the favourable cardiovascular profile and preservation of respiratory function [5, 6]. To our knowledge, this is the first description of successful use of esketamine combined with sevoflurane anaesthesia for TURP in severe thoracolumbar kyphosis.
A 73-year-old male (weight 55 kg, ASA status III) was scheduled to undergo TURP due to benign prostatic hyperplasia accompanying the symptoms of urinary urgency and frequency. The patient reported a long-standing history of uncontrolled ankylosing spondylitis and rheumatoid arthritis (Figure 1) and well-controlled hypertension. Chest CT and X-ray demonstrated kyphosis accompanied by thoracic deformity, while no abnormalities were found within the major cardiopulmonary structures (Figure 2). Pulmonary function tests were performed and found that forced vital capacity (FVC) was 1.12 L (38.7% of the predicted value), and the forced expiratory volume in one second was 1.09 L (48.8% of the predicted value), suggesting severe restrictive ventilatory defect. Echocardiography showed no obvious lesion or left ventricular diastolic dysfunction, and the electrocardiogram showed sinus rhythm with significant findings.
FIGURE 1
Plain radiograph of thoraco-lumbar kyphosis with visible severe kyphosis (approximately 90°) with a bamboo spine appearance and gross fusion of all the vertebrae
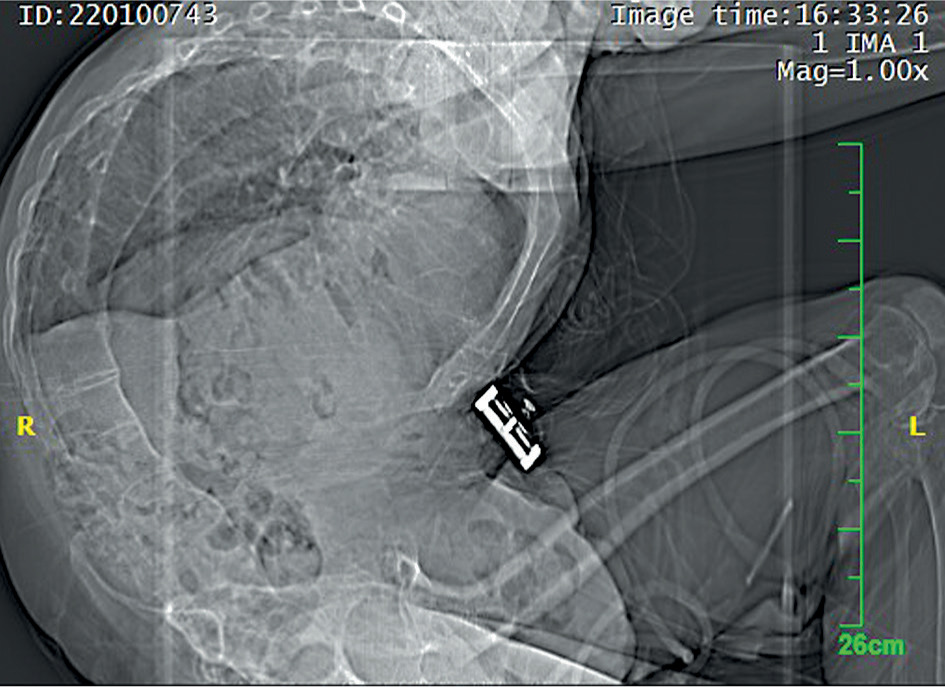
FIGURE 2
Position during surgery and anaesthesia. The anaesthesia under spontaneous breathing using esketamine combined with sevoflurane was performed successfully for the patient in the lithotomy position

The results of blood biochemical assays were within the acceptable range, including normal renal and liver function. Difficult airway of the patient was anticipated, due to Mallampati class IV, mouth opening < 3 cm, and extension and flexion limitation of the neck.
The patient and his family agreed and signed an informed consent form for the publication of the present case study. The current study was approved by the Ethics Committee of the Yancheng First People’s Hospital. Then the anaesthesia scenarios, anticipated difficulties, potential impending dangers, and outcomes of anaesthesia were explained to the patient. Considering the potential difficult airway, a consensus was reached between the patient and doctor: attempting conventional intraspinal anaesthesia first, and if that failed, proceeding to general anaesthesia alternatively. In the operating room, the patient was monitored using 5-lead electrocardiography, pulse oximetry, invasive blood pressure monitoring, and pure oxygen at a flow rate of 3 L min–1 was delivered by facemask. After establishment of vital signs monitoring, 0.4 mg penehyclidine hydrochloride was injected intravenously to minimize the respiratory secretions, light sedation was achieved by infusing a loading dose of dexmedetomidine (1 μg kg–1 h–1, 10 μg) over 10 min followed by maintenance dose (0.5 μg kg–1 h–1, 45 μg) for 90 min. Considering the patient’s long-term kyphosis and severe calcification of the hip and knee joints, the lumbar puncture was performed in a modified left lateral decubitus position with curved posture. During the operation, the head of the bed was raised to 40–50°, and the patient was placed in a “V” position supported by a pillow to fully fit the patient’s spine curvature. Considering that the V-shaped position made it difficult to deliver oxygen with a facemask, a surgical pad was placed on the patient’s right back to tilt the patient’s upper body slightly to the left, which enabled the convenience of the emergency oxygen treatment. Although general anaesthesia was the last scenario, we also prepared related equipment for difficult airway (including laryngeal mask, visual laryngoscope, fibreoptic bronchoscope, emergency tracheotomy kit). The anaesthesia was performed by a senior anaesthesiologist. After several failed attempts, the epidural needle finally entered the suspected epidural space, an epidural catheter was indwelt, and 3 mL of 2% lidocaine (60 mg) was injected as epidural test dose. No obvious adverse reaction was observed, then 15 mL of a 0.5% ropivacaine (75 mg) was injected in increments. However, this block failed with acupuncture tests showing sensory block at L2 level and no motion block detected on either side. We inferred that the abnormal curvature of the spine resulted in the inadequate block. Considering the difficult airway (Mallampati class IV and limited neck motion) and cardiopulmonary functional deficits, as well as large haemodynamic fluctuations at that time, general anaesthesia, with spontaneous breathing maintained, was commenced
A small dose of esketamine (0.3 mg kg–1, 16.5 mg) combined with 1~2% sevoflurane delivered by facemask ventilation in 100% O2 was chosen. The facemask was sealed around the mouth and nose by medical tape. The patient was kept in a state of anaesthesia throughout the 90-min operation, and an additional dose of esketamine (0.3 mg kg–1,16.5 mg) was administered as required to maintain anaesthesia according to body movement response. No muscle relaxants were used throughout the perioperative period. The anaesthesia machine was set in the autonomous breathing mode, with the tidal volume of 300–450 mL, respiratory rate of 12–24 per minute, and peak airway pressure of 10–20 cmH2O. The patient’s haemodynamic stability was kept within the range of 20% fluctuation of the baseline value. No respiratory depression or other intraoperative complications were observed during surgery. The operation was completed successfully.
We present here the successful management of anaesthesia for transurethral prostatectomy in severe AS with esketamine in combination with facemask delivery of sevoflurane under the circumstance of the extreme difficulty in neuraxial blocks and unavailability of general anaesthesia with endotracheal intubation, which provides a novel approach of anaesthesia to the established clinical problems in AS, and a significant learning point for other anaesthesiologists.
Patients with ankylosing spondylitis can present tremendous challenges in both general anaesthesia and neuraxial blockade. General anaesthesia is considered to be contraindicated in patients with AS and secondary deformity of the thoracolumbar spine, because of respiratory disease and disorders, cardiovascular embarrassment, and difficulty in airway management [7]. Due to immobilization of the cervical spine and possible temporomandibular joint disease caused by synovial hyperplasia and replacement of the fibrocartilage with fibrous tissue in AS [3], serious airway injury may occur during intubation for general anaesthesia. Meanwhile, thoracic deformity often affects lung morphology and function, which causes insufficient pulmonary function and consequent difficulty in oxygen supply during induction and intolerance of deoxygenation during extubation. Long-term breathing with a tube can also induce life-threatening conditions such as pulmonary infection, ventilator syndrome, cardiopulmonary interference, etc. Therefore, effective face mask ventilation becomes essential for safe airway management during general anaesthesia with difficulty in endotracheal intubation. Face mask ventilation can be lifesaving in a situation where the placement of a secure airway device proves to be challenging. Face mask general anaesthesia induction with sevoflurane has been reported in patients with a difficult airway [8]. Here we reported for the first time face mask general anaesthesia inhalation with sevoflurane in addition to esketamine for an AS patient undergoing TURP. This technique should be considered as an alternative anaesthesia approach in AS patients when a difficult airway is encountered.
As is known, patients undergoing transurethral resection of the prostate are generally elderly, may have pre-existing comorbidities, such as coronary artery disease, congestive heart failure, cerebrovascular disease, and respiratory disease and disorders including chronic obstructive pulmonary disease, as well as obstructive sleep apnoea, etc. Meanwhile, there are several risks and potential complications specific to transurethral resection of the prostate (TURP), including TURP syndrome, massive haemorrhage, perforation of the bladder and urethra, and prostatic capsular perforation. Spinal anaesthesia is often considered as the first choice for prostatectomy, which is beneficial to early diagnosis of TURP syndrome [9]. Furthermore, some researchers argue that significant haemodynamic changes in a lithotomy position will be affected more by general anaesthesia than neuraxial blockade [10, 11]. That is why in our case neuraxial blockade was chosen as the first anaesthesia scenario. However, neuraxial blockade failed eventually after the failure of attempted epidural anaesthesia. Some confounding factors may contribute to the failure of neuraxial anaesthesia. First, the destruction and rebuilding of spinal bone caused by acute and chronic spondylitis may result in fibrosis and ossification of the intervertebral disks, ligamentum flavum, sacroiliac joints, and costovertebral and facet joints [3]. Several studies reported that spinal anaesthesia was successfully achieved through both midline and paramedian approaches in AS patients [3, 12]. However, the success rate was lower in epidural anaesthesia, possibly due to the larger size of the needle. Second, the epidural space may disappear in patients with severe deformity of the thoracolumbar spine, because of extreme stretching of the ligaments as well as the dura and arachnoid mater. In such cases, the signs of successful epidural puncture, such as the difference in distensibility between the ligamentum flavum and the epidural space and the existence of negative pressure within the epidural space, no longer exist [13]. Therefore, neuraxial blockades pose a great risk of inadvertent dural/arachnoid puncture, which may lead to cerebrospinal fluid outflow. In our patient, the placement of an epidural needle was extremely difficult, and the block failed even after the needle finally entered the suspected epidural space, with an indwelling catheter inserted. Our experience highlighted the importance of multiple anaesthesia scenarios in anatomically distorted thoracolumbar spine where technical difficulties in neuraxial blockades exist.
At the request of the patient and to avoid complications associated with epidural and spinal anaesthesia (spinal haematoma, neurological damage, etc.), no spinal puncture was performed again, and eventually esketamine was chosen as the leading drug of general anaesthesia with spontaneous breathing maintained during the operation.
Ketamine is a racemic mixture containing 2 optical isomers: S(+)-ketamine (esketamine) and R(–)-ketamine [14]. It is an antagonist of NMDAR, which facilitates dissociative anaesthesia as well as analgesia, while maintaining haemodynamic stability [15–17]. Moreover, epidural ketamine has been shown not to induce cardiovascular depression, and it is associated with beneficial effects such as preventing shivering, obturator nerve reflex, nausea, and any other adverse effects, which suggests ketamine should be an advantage in urological surgery of patients with cardiopulmonary diseases [6, 18, 19]. Esketamine is a right-handed split of ketamine. Its anaesthetic potency is approximately three times higher than (R) ketamine, and about twice as potent as the that of racemic mixture [20]. Esketamine causes little interference to respiration and circulation [5], less impairment to cognitive functions and memory, and is associated with faster recovery. One Chinese cohort study showed that a single dose of 0.5 mg kg–1 of esketamine was both safe and well tolerated in Chinese patients with no serious adverse events, which confirms its efficacy and feasibility for routine surgical anaesthesia [5]. In this case, we chose general anaesthesia using esketamine combined with sevoflurane inhalation with spontaneous respiration maintained. The patient received a total of 35 mg esketamine during the operation and remained unconscious throughout the procedure. The haemodynamic parameters remained stable during the perioperative period, and no postoperative adverse reactions were reported. The patient was discharged 7 days after the operation.
In conclusion, low-dose esketamine combined with sevoflurane inhalation, with spontaneous breathing maintained, can be used as an alternative anaesthesia for TURP in elderly patients, especially in cases with severe thoracolumbar kyphosis where technical difficulty in central neuraxial block placement exists.