







Introduction
The pain experienced by patients with chronic wounds is multi-causal [1]. Pain symptoms may be classified as: pain that is felt continuously; incidental pain that occurs during daily activities; procedural pain (e.g. dressing change) and pain associated with significant intervention in the wound, e.g. during deep cleansing [2]. The severity of pain is usually associated with many factors, including psychosocial factors, such as age, gender, education, mental state, as well as environmental factors such as the duration of the procedure or the waiting time for the procedure. It has been proven that the wounds of patients in distress heal 24% longer than the wounds of patients not under the influence of stress, which may cause prolonged hospitalization [3].
Recent theories emphasize the role of the environment in the sensation of pain [4]. Six consecutive studies on the influence of the environment on the perception of pain showed a significant reduction in pain intensity when patients listened to music or watched visual projections [5]. It is also known that virtual reality methods significantly reduce the intensity of pain and the level of anxiety during dressing changes [3]. Patients who received audio-visual distraction used less sedatives and reported less pain. Hoffman, Patterson, and Carrougher proved that patients who reported a high level of empathy with the Virtual Reality (VR) environment showed the greatest reduction in pain and anxiety [3].
The use of eye-tracked games is an issue that has been known for many years [6]. However, the use of this technology in relation to pain reduction in e.g. the management of chronic wounds is not a well-described topic. In this approach, the use of eye tracking can be compared to the use of virtual reality (VR) technology, which is successfully used to distract the patient (e.g. during a dressing change, during painful rehabilitation) [7–12]. Thus, it can be argued that the use of eye tracking can be a very useful technique during nursing work related to wound management.
Aim
The aim of this work was to assess usability of eye-tracked games distracting the patient during wound management activities in an outpatient surgical clinic and therefore verify if it is worth introducing eye trackers into daily clinical routine.
Material and methods
Patients inclusion
Forty patients consecutively registered for an appointment at the outpatient clinic were qualified for the study. Patients were included during the period between 1.09.2021 and 15.10.2021. Patients were informed in an accessible way about the purpose and essence of the study. Patients were informed about the possibility of withdrawing from the study at any stage of its duration without any influence on the treatment process. Patients gave informed consent to participate in study.
Survey
A self-administered questionnaire was used, which consisted of four parts: 1) demographic data, 2) pain level daily 3), pain level during dressing change and 4) pain level with eye trackers. The study consisted of 11 closed questions. The survey was anonymous. Only printed surveys were used. Excel (Microsoft) was used for data collection and pre-processing.
Eye-tracking games
Eyetracker PCEye 5 gen (Tobii Dynavox LLC.) was used (Figure 1) on a regular laptop (USB connected). Every patient had eye tracker validated to obtain more precise piloting. Look to learn (Smartbox) application was used to distract pain. Patients played the game “throwing cakes into faces” (Figure 1 A). The aim of throwing cakes was to target the face by eye movement and gaze to throw a cake. The patient was sitting or lying depending on wound position and general condition (Figures 1 B, C). A laptop was on a surgical table and patients did not touch the laptop or the eye tracker which allowed the patient to support lying/sitting position (Figure 1 D).
Figure 1
Application of the eye tracker technology in patients with chronic wounds. A – General appearance of the eye tracker device and the computer – throwing cakes into faces. B – The example of a sitting patient. C – the example of a lying patient. D – laptop with an eye tracking device placed on a surgical table

Time
Time of dressing change with eye tracker was compared to time needed for dressing change without the device.
Nurse opinion
Two nurses were included in the study in order to obtain information about pros and cons regarding using eye tracking games.
Statistical analysis
All tests were performed with the Statistica 12 software. The distribution was analysed with the Shapiro-Wilk test and the equality of variance was checked with the Levene’s test. Kruskal-Wallis and U Man-Whitney tests were used. The significance level was set at 0.05 (5%). Twenty-four of patients (60%) were already hospitalized in our Hospital.
Results
Forty patients with non-healing wounds were included into the study (all patients were > 41 years old). The majority of surgical clinic patients were people > 71 years old (53%) (Table 1), with vocational, nonmedical education (93%), male (n = 22). Most patient had their wound not healed for less than 1 year (40%), followed by a non-healing period of 1–2 years (33%).
Table 1
Basic data of the group of examined patients
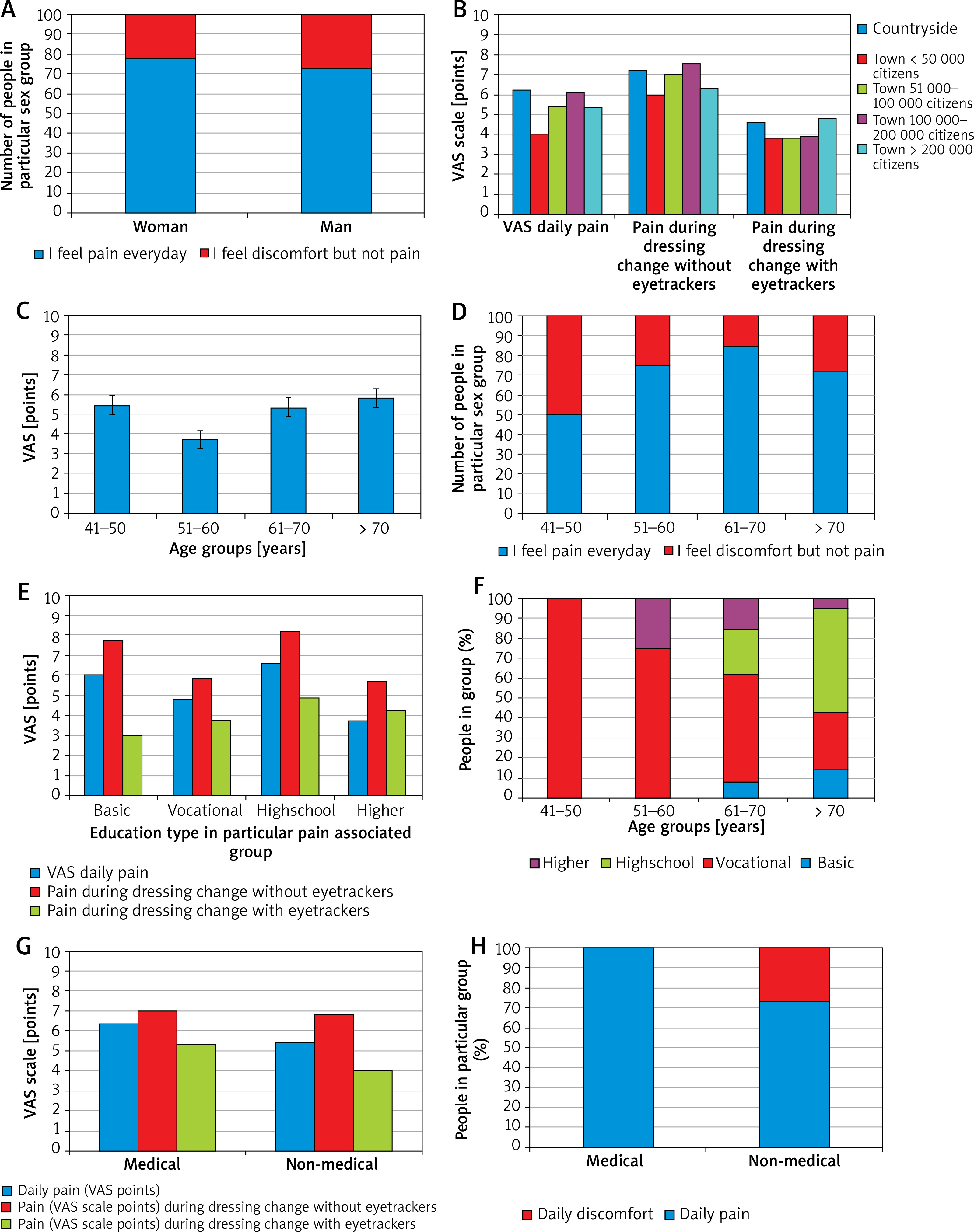
Most frequently patients declared daily VAS 5 pain level (min. 2, max. 10) and 53% of them had to intake pain killers daily. Seventy-five percent of respondents declared that they feel pain every day, other 25% of patients feel discomfort but not pain. There were significant differences between answers about daily sensation of pain or discomfort and level of pain measured by the VAS scale without eye trackers (p = 0.004) and with eye trackers (p = 0.03). Age, sex, and place of living had no impact on the daily level of pain or pain level during dressing change both without and with eye trackers. Place of living was a parameter that had no impact on attitude towards eye trackers or impact of eye trackers on pain decrease. Lowest everyday pain sensation was in the 41–50 years old group – 50% of respondents declared everyday pain, however average daily VAS point in this group was still 5.5. However, the lowest average VAS points (3.8) were in the 51–60 years old group. The highest average daily pain was observed in people living in countryside. Pain levels during dressing change with and without eye trackers were second in the group living in countryside. Education level had a significant impact on daily pain sensation (p = 0.0127) and pain sensation while dressing change without eye trackers (p = 0.0366), but not with eye trackers. Differences between the place of living and education level were insignificant, but there was a difference between age and education level (p = 0.0224) (Figure 2).
Figure 2
The degree of pain perceived by patients on the VAS scale. A – Daily pain sensation depending on the gender of the patient; B – daily pain sensation depending on the place of living; C – daily pain sensation depending on the age group; D – percentage of patients’ pain sensation depending on the age; E – pain level depending on the level of education; F – type of education in particular groups; G – pain level depending on the type of education; H – daily pain or discomfort level depending on the level of education
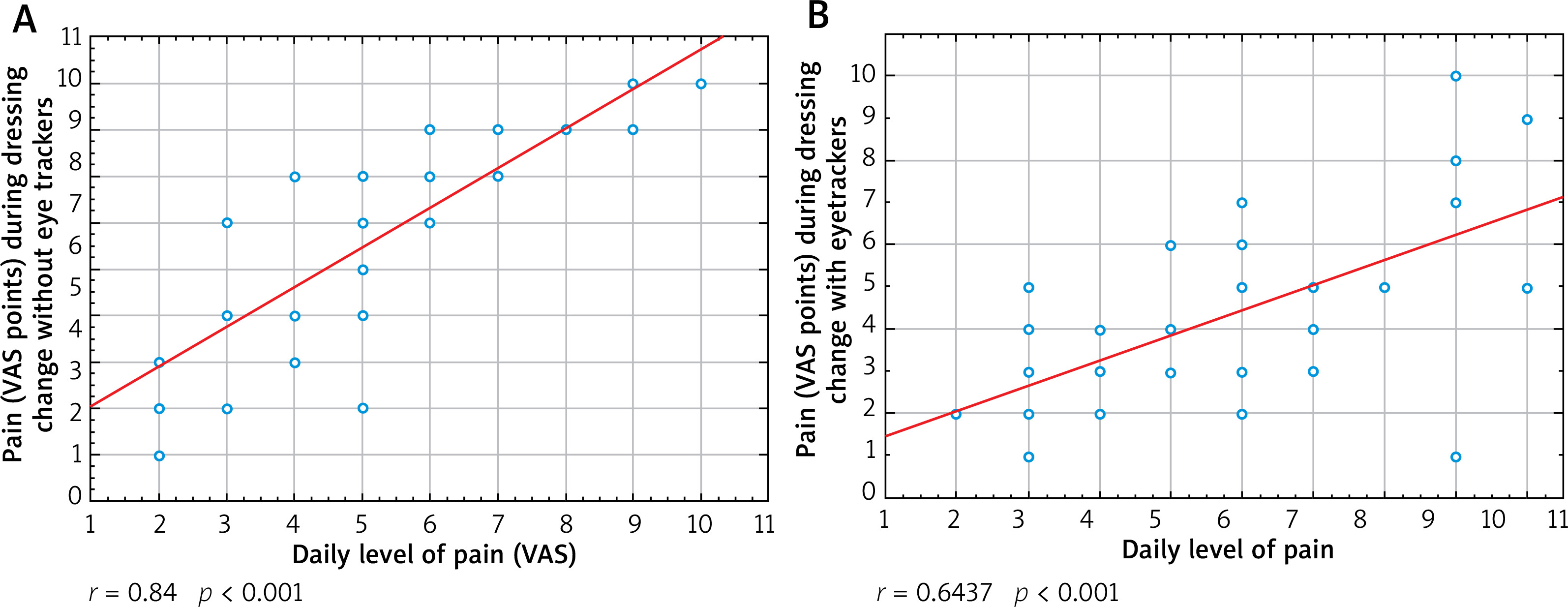
There was a high correlation between daily pain sensation (in VAS scale) and pain during dressing change without eye trackers (r = 0.84; p < 0.001). Correlation between daily pain and pain during dressing change with eye trackers was medium (r = 0.64; p < 0.001) (Figure 3).
Figure 3
The impact of eye tracking games on pain sensation during the dressing change; A – the correlation between daily pain sensation (in VAS scale) and pain during dressing change without eye trackers; B – correlation between daily pain and pain during dressing change with eye trackers
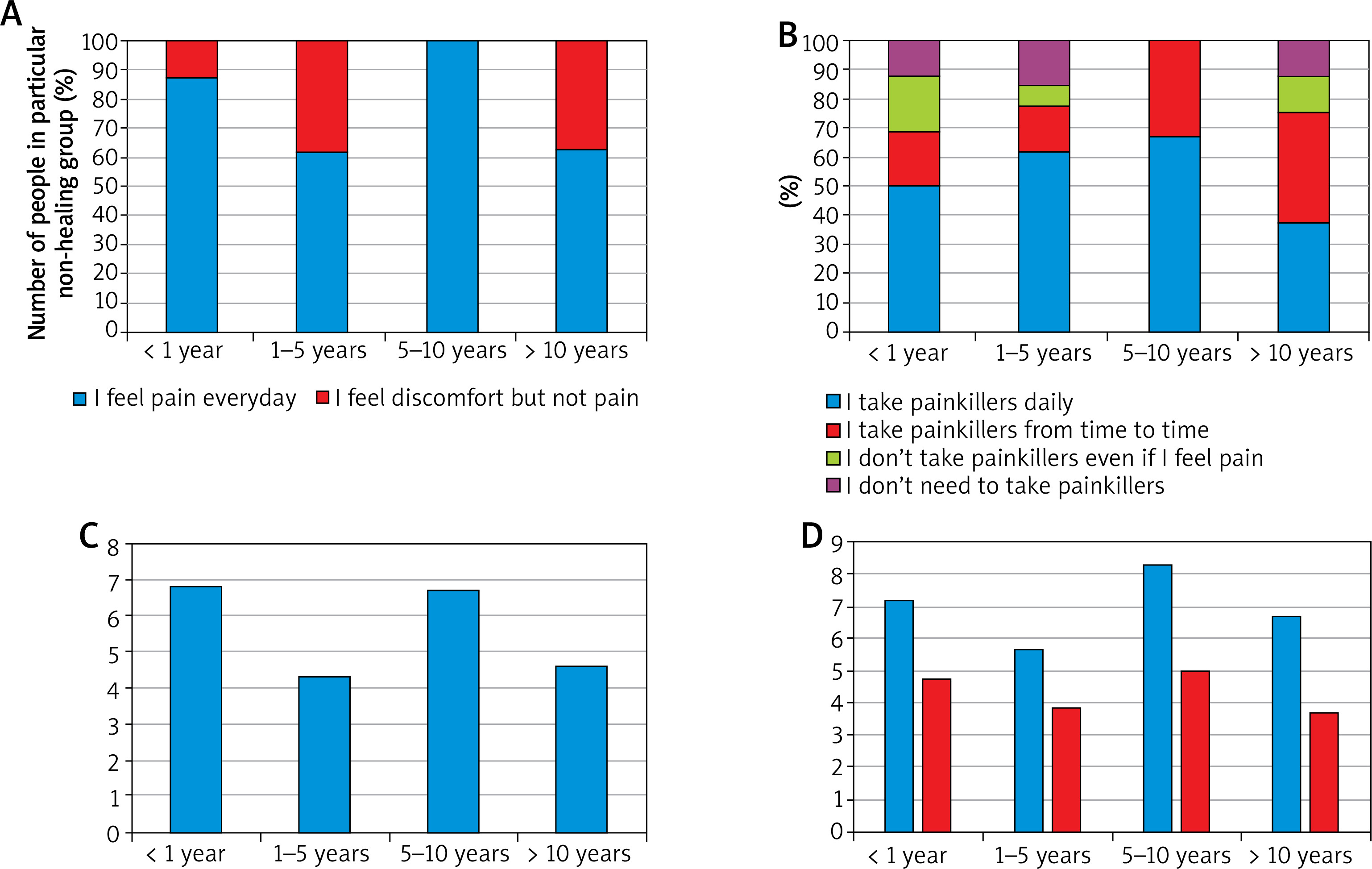
There were significant differences between length of non-healing and length of time of wound service in the outpatient clinic, but surprisingly the patients with wound present for more than 10 years were the group who was taken care of in the outpatient clinic for the shortest period of time (less than a month). The presence of constant pain or discomfort was depending on length of wound non-healing (p = 0.05), and VAS points were associated with length of non-healing period of wound (p = 0.0452). The level of pain during dressing change without eye trackers was significantly associated with length of the wound non-healing period (p = 0.0324) but not with eye tracker. The range of pain without eye trackers was 5.7–8.3. The lowest pain level was noted in the group with wound open for 1–5 years and highest in 5–10 years. Whereas the level of pain with eye trackers was similar (3.7–5) in every age group and highest in 5–10 years (average 5 VAS points) (Figure 4). There was also a medium correlation between pain level without eye trackers and with eye trackers (p = 0.618; p < 0.001). Length of the non-healing period was not a parameter associated with attitude toward eye trackers.
Figure 4
The level of pain or discomfort during the period of wound healing: A – daily pain sensation depending on the length of wound non-healing period; B – painkiller intake depending on the length of the wound non-healing period; C – VAS daily pain depending on the length of the wound non-healing period; D – VAS daily pain depending on the length of wound non-healing period
Routine painkiller intake was also not impacted by time of presence of non-healed wound nor with time of wound management in the outpatient clinic.
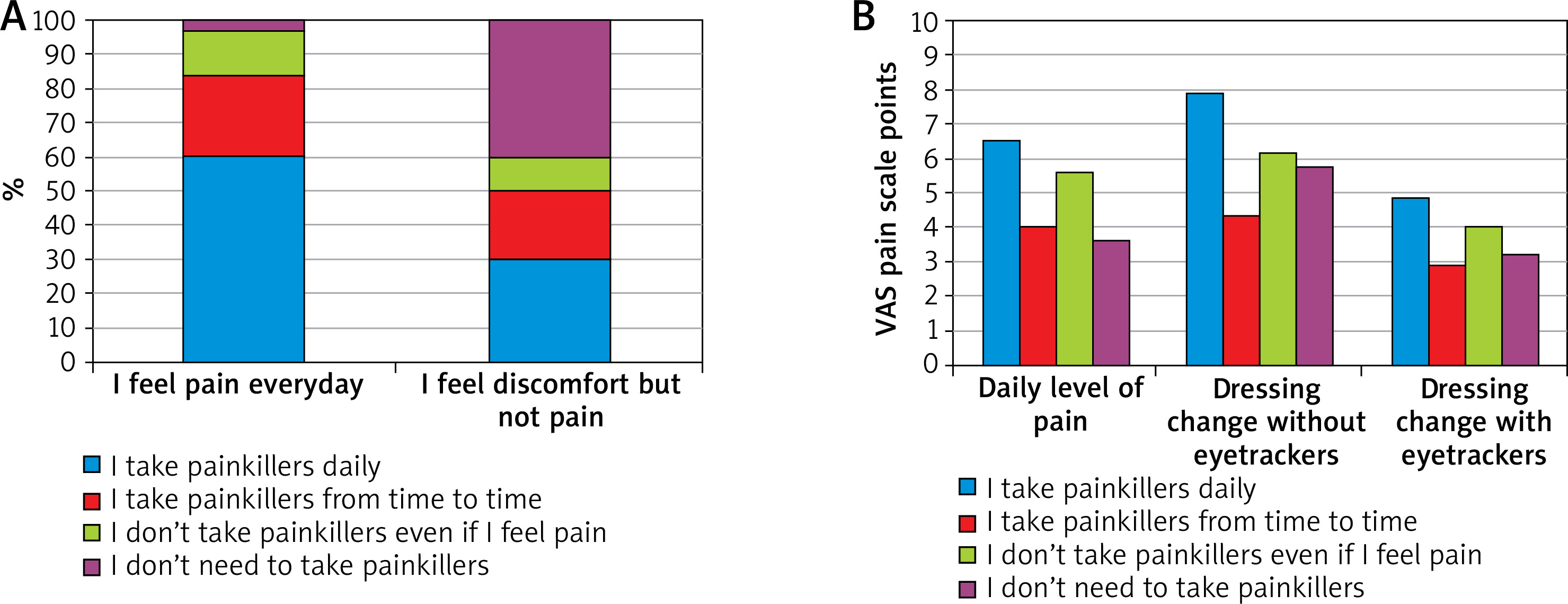
The level of painkiller intake was associated with daily pain/discomfort sensation (p = 0.0268) and with daily VAS points scale (p = 0.0121). Daily pain sensation was not the factor that had an impact on feeling if eye trackers should be routinely used in the outpatient clinic. Discomfort or pain sensation during dressing change was associated with daily painkiller intake (p = 0.0378). Also VAS points during dressing change without eye trackers were associated with daily painkiller intake (p = 0.0256). The level of pain (VAS points) during dressing change without eye tracker was not associated with daily painkiller intake (Figure 5).
Figure 5
Painkiller intake among patients with chronic wounds; A – painkiller intake depending on daily pain sensation; B – painkiller intake depending on the level of pain
Thirty-seven (93%) of respondents declared that using eye-tracking games during dressing change is a good idea. There was an association between decreased pain sensation with eye trackers and feeling that eye trackers should be used routinely in the surgical clinic (p = 0.0195).
The average time of dressing change was 20 ±14 min. Visits where eye tracker was used for the first time lasted on average 28 ±6 min. This was time needed for explanation of the whole procedure and to calibrate the eye tracker for a particular person. No violent behaviour, including swearing was noted during using eye tracker.
Discussion
The main goal of this study was to verify the usability of eye-tracked games in a group of chronic wound patients. The purpose of the usage of such device was to distract the patient’s attention during wound management activities. In this approach the subjective pain sensation would be decreased as the patient was not focused on the painful wound care activities. However, it should be remarked that the usage of eye tracking games in this particular approach is not a well-described topic in the literature. The lack of suitable data could make it difficult to discuss the obtained results. But on the other hand, the deficit of suitable literature creates the niche for further research and adjustments.
There is a similar technology that found its application in multiple medical procedures – virtual reality (VR). The use of VR is becoming an increasingly acceptable solution in the field of many medical protocols (venous access, dental care, oncological care, dressing change in burn patients or as exposure before elective surgery under general anaesthesia, post-burn rehabilitation) [7–12]. VR helps to reduce the experience of pain by shifting attention during therapy sessions by moving the patient into a three-dimensional virtual world. Thus, the VR allows patients to go for a virtual walk via a 180-degree projection, fully interacting with the environment [7–12]. Of course it could be argued that the fact that VR technology introduces the patient to the closed imaginary world is the main advantage of that technology. While eye tracking games are only able to focus the patient’s attention on the screen without the real detachment from the reality. But accordingly to our findings that it is not necessarily the disadvantage of eye tracking games. Our major observation was the fact that eye tracking games were able to significantly decrease the level of pain during the dressing change in the studied group of patients. Additionally, patients did not touch the device at any stage of the procedure. On the one hand, it would significantly reduce the need for ongoing sterilization protocols of the device. And on the other hand, no need to use patient’s hands to proceed would enable the eye tracking games to be used in patients with burned hands or disabled hands.
Based on the analysis of the age of the studied patients it could be argued that 67% of female and 41% of male patients were older than 70 years old. The majority of the patients suffered from their chronic wounds for at least 1 year (Table 1). Chronic wounds are described as wounds that are unable to heal by the body’s natural healing process [13, 14]. Failure to treat chronic wound understood as less than 30% wound closure in 4 weeks after treatment [13] affects approximately 8 million people worldwide [15]. Age, diabetes, obesity, poor blood circulation, lack of angiogenesis, neuropathy, risk of infection or persistent inflammation support the increasing prevalence of chronic wounds [13, 16]. A multidisciplinary approach is needed. Surgeons, internal medicine specialists, infectious disease specialists, diabetologists, specialty nurses and basic scientists are listed as needed to manage chronic wounds [17]. However pain is often studied only in the aspect of quality of life. It is well known that pain has an impact on quality of life [18], but it also has to be included in the multidisciplinary approach. Wound-related pain is often under-assessed and may therefore be suboptimally managed. Pain impairs mobility, which can decrease effective vascular circulation and this may retard tissue perfusion hampering wound healing [19]. Serena et al. claims that that men and women react to pain differently [20], however in our study, pain was sensed by 78% of women and 73% of men, while the rest of the group declared daily discomfort but not pain (Figure 2). There was no single person who declared lack of discomfort or pain. It was found hard to assess the impact of age on pain as some studies indicate older adults are more sensitive to pain, whereas others suggest a decrease in sensitivity with age [21, 22]. The results obtained in this study showed that the group of the youngest patients (41–50 y.o.) did not suffer from daily pain as severely as patients in older groups (Figure 2). The situation of daily pain was the worst in the group of patients aged 61–70 years (Figure 2). The problem of constant feeling of chronic pain necessitates the use of painkillers (Figure 4). The results of the studies show that 60% of patients who report chronic pain take painkillers every day. In contrast, patients complaining of discomfort (but not pain) constituted 30% of patients who used painkillers continuously, while the remaining patients did not use these drugs at all or on an ad-hoc basis (Figure 5). In this manner the usage of eye tracking games lead to a significant pain reduction during the dressing change (Figure 3). It could be concluded that pain medications are suitable for taking control of patients’ chronic wound pain during medical protocols, but an exploration of eye tracking games could be able to reduce the sensation of pain by distracting the attention of the patient. Similar conclusion comes from works of other authors that used the VR in order to put the brain into divided attention from their acute pain [7–12].
It should be also remarked that eye tracking is inexpensive and widely available on the global market. Eye tracking can be a non-pharmacological analgesic treatment for the pain that accompanies wounds of various origin. In accordance with the results obtained in this paper, the usage of eye tracking games should be a routine protocol in e.g. an outpatient surgical clinic as it has been verified as worth being introduced into daily clinical routine.