





The COVID-19 pandemic has produced the greatest global biological threat in the 21st century. On 11 March, 2020, the World Health Organization declared coronavirus disease 2019 (COVID-19) a pandemic [1]. As of 17 October, 2020, almost 40 million cases of this new disease, and 1.1 million deaths, have been reported worldwide [2]. Seven months later, on 15 May, 2021, these figures had increased to 162 million cases and 3.4 million deaths, respectively [3]. The pandemic has affected all continents, but the number of cases and deaths varied in different regions of the world [2, 3].
A significant proportion of patients admitted to the hospital due to COVID-19 requires intensive care unit (ICU) admission. ICU mortality in patients with this disease is relatively high, but the range of reported mortality rates is broad. Death rates are influenced by the local structure of the healthcare system, the quality of ICU care, and the learning curve effect [4–6]. In a systematic review and meta-analysis on this topic, meta-regression by the month of publication revealed a significant reduction in the reported mortality rates over time [6]. On the other hand, COVID-19 transmissibility, morbidity and mortality may be increased by the emergence of new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants [7].
In Poland, the first positive case of COVID-19 was diagnosed on 4 March, 2020; on 20 March, 2020, a state of COVID-19 pandemic was announced [8]. Selected multidisciplinary hospitals were converted into designated infectious disease centres [9]. Initially, the disease spread was well controlled due to the prompt adoption of social distancing and complete lockdown throughout the country [10]. In the following months, the situation remained stable, but the number of new cases and deaths dramatically increased in September 2020. This was considered a “second wave” of the pandemic in Poland. As of 17 October, 2020, 149,903 cases and 3,308 deaths have been confirmed in Poland [2]. As it turned out later, this was merely a mild prelude to the further events that followed during the “third wave” of the pandemic, when the United Kingdom (UK) variant became dominant in Poland. As a result, on 15 May, 2021, pandemic indices increased to 2,851,911 cases and 71,609 deaths and Poland became a country with extremely high mortality from COVID-19, based on the number of inhabitants [11].
Apart from our previous study (covering only a part of the first pandemic wave and aiming at the comparison of patients admitted to the ICU with those disqualified from ICU treatment) [8], no reports analysing ICU patients with COVID-19 in Poland are currently available. According to our data, it is clear that the mortality rate in this group of patients is alarmingly high. However, it is still not known what determines the survival or death of these patients in Polish hospitals. For various reasons, these factors may be different from those observed in other countries [12].
Therefore, in our study, we aimed to identify independent risk factors for ICU death among patients admitted to the ICU due to COVID-19 during one year of the pandemic in a large multidisciplinary, COVID-dedicated hospital located in the Silesian region of Poland.
METHODS
In this retrospective, single-centre study, we analysed the data of all consecutive patients with COVID-19 infection, who were treated in the ICU and completed their ICU stay in the biggest COVID-19-dedicated hospital in the Silesian Region of Poland at that time. Data of all patients with COVID-19 infection, treated in the local ICU between 10 March, 2020 and 10 March, 2021, were reviewed. All analysed patients spent their ICU stay in the Department of Anaesthesiology and Intensive Therapy in a Provincial Specialist Hospital in Tychy in the Silesian region of Poland between 10 March, 2020 and 10 March, 2021. This ICU (as well as the rest of the hospital) was transformed into a COVID-19 dedicated unit on 12 March, 2020. Hospital management of the Provincial Specialist Hospital in Tychy approved the use of patient data for scientific purposes. The Ethical Committee of the Medical University of Silesia in Katowice approved the study and due to its retrospective and anonymous nature, waived the need for consent of the patients to participate in the study.
The primary objective of this study was an extensive comparison of all available ICU pre-admission, admission, and treatment data between survivors and non-survivors of the ICU stay. The analysed data included: circumstances surrounding ICU admission, comorbidities, clinical status at ICU admission, laboratory results closest to ICU admission, antiviral medications and ICU procedures used in the process of treatment. The secondary objective was to identify these variables that had an independent influence on ICU death in this population.
We only analysed patients who met the following criteria:
the patient was hospitalised in the ICU at some point,
the patient completed the whole ICU stay (from the date of ICU admission to the date of ICU discharge or ICU death) between 10 March, 2020 and 10 March, 2021,
the patient had a SARS-CoV-2 infection, confirmed by real-time reverse transcriptase-polymerase chain reaction (RT-PCR) analysis from nasal and pharyngeal swabs or lower respiratory tract aspirates.
Analysed variables were assessed retrospectively. Comorbidities were identified based on data available in medical records, separately and in a combined form, as the Charlson Comorbidity Index [13]. Patients were also considered frail when they obtained ≥ 5 points on the Clinical Frailty Scale [14].
Continuous variables were presented as mean and standard deviation, while categorical variables were presented as percentages. Univariable logistic regression was used to test for statistical significance. Circumstances surrounding ICU admission, comorbidities and clinical status at ICU admission (listed in Table 1) as well as laboratory results closest to ICU admission, antiviral medications and ICU procedures used in the process of treatment (listed in Table 2) were compared between survivors and non-survivors of ICU stay. A progressive stepwise method was then used to obtain a reduced multivariate model. Variables with a P-value < 0.05 were then included in the multivariable logistic regression analysis, where P < 0.05 was considered as significant. On the basis of these calculations, independent risk factors of ICU death were identified in this group. Additionally, Kaplan-Meier curves for the first 30 days of ICU stay were compared between patients considered to be frail or non-frail (≥ 5 or < 5 points on the Clinical Frailty Scale). Statistical significance was considered when a P-value was lower than 0.05. The analyses were performed and graphs were created using Statistica 13.0 (TIBCO Software Inc.).
TABLE 1
Circumstances, demographic data, comorbidities and clinical status at ICU admission
TABLE 2
Laboratory results closest to ICU admission, antiviral medications and ICU procedures
RESULTS
Between 10 March, 2020 and 10 March, 2021, 113 adult patients with confirmed COVID-19 infection were admitted to the ICU and completed their ICU stay with either discharge or death. There were 73 deaths in this group; therefore, the ICU mortality rate was 64.6%.
Comparison of circumstances surrounding ICU admission, comorbidities and the clinical status at ICU admission between non-survivors and survivors is presented in Table 1. Mean hospital stay before ICU admission was significantly longer in non-survivors of ICU stay (4.8 ± 4.7 vs. 3.0 ± 3.9 days, P = 0.048). Non-survivors were also significantly older (64.6 ± 9.5 vs. 60.0 ± 12.8 years, P = 0.036), but the percentage of patients aged over 65 years in both groups was similar (43.8% vs. 47.5%, P = 0.860, respectively). In the whole analysed population, the majority of patients were male (68.1%), but the percentage of male patients was similar between non-survivors and survivors (P = 0.918). Mean body mass index (BMI) in all patients was 30.7 ± 6.8 kg m-2 (from 20.2 to 55.4 kg m-2), and the mean BMI values were not significantly different between non-survivors and survivors (30.2 ± 6.4 vs. 31.8 ± 7.5, P = 0.236, respectively). Distribution of blood groups had no relationship with ICU mortality.
Regarding comorbidities, a significant difference regarded only patients with chronic renal failure (26.0% vs. 5.0%, P = 0.013) and the percentage of the remaining comorbidities was similar in both groups (Table 1). Non-survivors had a marginally higher mean Charlson Comorbidity Index (5.9 ± 3.6 vs. 4.5 ± 4.1 points, P = 0.063) and a higher mean Clinical Frailty Score (4.8 ± 1.5 vs. 3.9 ± 1.4 points, P = 0.004). The percentage of patients considered to be frail (Clinical Frailty Scale equal to or exceeding 5 points) was higher among non-survivors (57.5% vs. 30.0%, P = 0.009).
The clinical status of non-survivors and survivors at ICU admission was broadly similar (Table 1). A significant difference was observed in the mean first recorded oxygen saturation, which was extremely low in both groups, but was significantly lower in non-survivors (mean 66.8 ± 19.5 vs. 74.2 ± 13.4%, P = 0.037) and also significantly more patients in this group had their first recorded oxygen saturation lower than 70% (49.3% vs. 25.0%, P = 0.021). Almost all patients (98.6%) in the non-survivors group required inotropic support already at ICU admission, in comparison with 82.5% in patients who survived their ICU stay (P = 0.005).
The difference between non-survivors and survivors in their mean admission ICU scoring was also significant. The mean admission APACHE II score for the whole ICU population of patients with COVID-19 was 21.6 ± 8.0 points, while the mean APACHE II score in non-survivors vs survivors was 22.9 ± 7.9 vs. 19.0 ± 7.8 points, respectively (P = 0.017). The mean SAPS II scoring for the entire population was 59.3 ± 17.9 points, while the mean SAPS II score in non-survivors vs. survivors was 62.1 ± 18.1 vs. 54.0 ± 16.7 points, respectively (P = 0.023).
The ICU mortality rate for all patients was 64.6%, but the expected mortality for the admission APACHE II and SAPS II score was 42.7% and 37.7%, and therefore the observed to expected (O/E) mortality ratio for admission APACHE II and SAPS II score was 1.51 and 1.71, respectively.
Laboratory results closest to ICU admission, antiviral medications and ICU procedures are presented in Table 2. Non-survivors were more likely to have admission lactate plasma levels > 2.0 mmol L–1 (61.6% vs. 35.0%, P = 0.012), procalcitonin (PCT) > 2.0 ng mL–1 (17.8% vs. 2.5%, P = 0.039) and plasma protein < 50 g L–1 (34.2% vs. 5.0%, P = 0.001). Regarding antiviral medications, there were significantly more patients taking arechine/chloroquine, lopinavir/ritonavir and convalescent plasma among survivors (P = 0.027, 0.028 and 0.015, respectively).
All analysed patients were intubated and invasively ventilated during their ICU stay. Out of all 113 patients, 52 patients were already invasively ventilated on ICU admission. In 59 patients invasive ventilation was started within one hour of admission to the ICU. In the remaining 2 patients invasive ventilation was started a few days after the ICU admission. Non-survivors were marginally less likely to assume the prone position during mechanical ventilation (19.2% vs. 37.5%, P = 0.056), with 58.9% of non-survivors and 77.5% of survivors requiring tracheostomy (P = 0.075). Inotropic support was used more frequently among non-survivors (98.6% vs. 82.5%, P = 0.005). Renal replacement therapy was used in 23.3% of non-survivors and 12.5% of survivors (P = 0.256). Eight patients were given do-not-resuscitate orders before death in the non-survivors group.
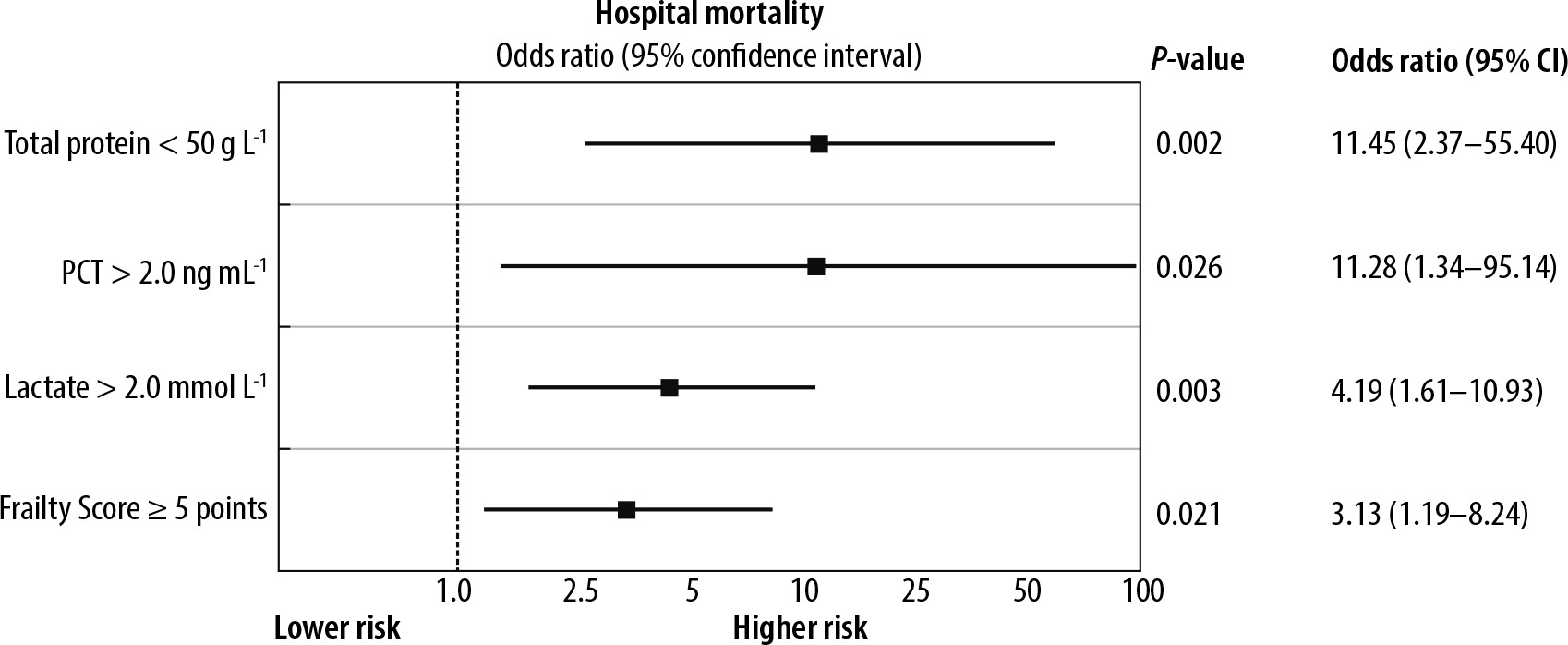
Overall, based on data from Table 1 and 2, there were 11 factors differentiating non-survivors from survivors in the univariable analysis. Factors that independently influenced ICU death, however, were limited to: admission total protein < 50 g L–1 (OR = 11.5, 95% CI: 2.4–55.4, P = 0.002), admission PCT level > 2.0 ng mL–1 (OR = 11.3, 95% CI: 1.3–95.1, P = 0.026), admission lactate level > 2.0 mmol L–1 (OR = 4.2, 95% CI: 1.6–10.9, P = 0.003) and Clinical Frailty Score ≥ 5 points (OR = 3.1, 95% CI: 1.2–8.2, P = 0.021). The results of the multivariable analysis are presented in Figure 1.
Patients considered frail (≥ 5 points in a Clinical Frailty Scale) had significantly worse survival curves in the first 30 days of ICU stay in comparison to the remaining ICU patients with COVID-19 infection (P = 0.002). Comparison of Kaplan-Meier curves in patients considered to be frail or non-frail is presented in Figure 2.

DISCUSSION
In our study, we confirmed that low total protein, frailty, concomitant bacterial infection (described as procalcitonin level above 2 ng mL–1) and increased lactate levels at ICU admission were associated with ICU death among patients with COVID-19 infection.
Our data were obtained in the ICU of a busy, multidisciplinary hospital, located in an industrial area with a high population density. This ICU was quite typical for the Polish healthcare system. Importantly, the entire hospital was converted into a COVID-dedicated unit at the very beginning of the pandemic [8]. All our patients required invasive mechanical ventilation during their ICU stay. In a meta-analysis including 45 studies with 16,564 patients from 17 countries across four continents, invasive mechanical ventilation was required in 67.7% (95% CI: 59.1–75.7%) of cases [15].
The mortality rate among our analysed patients was almost 65%. Such a mortality rate in the ICU is alarmingly high, but we have been dealing with a very specific population. Apart from that, it has already been proved that the mortality rate in Polish intensive care units is generally higher in comparison to other European countries, but this is not due to the inferior quality of care. This issue has already been widely discussed in the medical literature [12].
The mean age of non-survivors in our study was significantly higher in comparison to survivors. This finding was not surprising because age is a well-recognised risk factor for fatal outcomes in patients with COVID-19. In a multicentre, prospective cohort study conducted in 138 hospitals in France, Belgium, and Switzerland, non-survivors treated in the ICU were, on average, 7 years older than survivors [16].
The majority of patients analysed in our study had various comorbidities before their admission to the ICU, most commonly arterial hypertension, diabetes mellitus, heart failure, coronary artery disease, and peripheral vascular disease. Numerous studies have confirmed that patients with existing chronic diseases were more likely to require ICU admission for COVID-19 infection than the rest of the population [16, 17]. This is confirmed in our observation, as only 8% of all our ICU patients did not have any comorbid disease.
To assess the aggregate effect of multiple comorbidities in our cohort, we used the Charlson Comorbidity Index [13] and the Clinical Frailty Scale [14]. Previous studies indicated that a Charlson Comorbidity Index score above zero was associated with an increased risk of severe COVID-19 and death in an age- and sex-adjusted analysis [17, 18]. In an interesting publication, aiming to find a simple scoring system for predicting mortality and determining severe disease, mortality risk of patients with a Charlson Comorbidity Index score above 2.5 was 10.7 times higher than in the remaining patients [19].
It turned out, however, that the frequency of comorbidities in our study was generally similar among non-survivors and survivors. The only exception was pre-admission chronic renal failure, occurring five times more often among non-survivors.
The majority of our patients were admitted to the ICU with profound hypoxaemia. Moreover, patients were either already mechanically ventilated or required mechanical ventilation shortly after ICU admission. The mean admission oxygen saturation in non-survivors was as low as 67%. These findings could have been expected, as the severity of hypoxaemia is an important predictor of ICU admission, risk of invasive ventilation and death in patients with COVID-19 [20]. Patients often develop so-called “silent” or “happy” hypoxaemia, without the typical accompanying symptoms (e.g., dyspnoea, tachypnoea, or hypercapnia); therefore, early recognition of very low oxygen saturation on arrival may have a profound impact on the outcomes of these patients [21].
The mean admission APACHE II and SAPS II scores in our patients were 21.6 and 59.3 points, and therefore the expected ICU mortality rates for this population were 42.7% and 37.7%, respectively [22, 23]. However, the observed ICU mortality was higher, approaching 64.6%. An early, single-centre study performed in Wuhan highlighted an ICU mortality rate of 62% in patients with a median admission APACHE score of 17 points [24]. According to the recent data coming from the Intensive Care National Audit and Research Centre (ICNARC) database, covering 7,864 patients with COVID-19 ventilated within the first 24 hours, the mean APACHE II score was 16 points and the mortality was 49% [25]. These results clearly show that the actual mortality rate in patients with COVID-19 infection may be much higher than that predicted based on the most common ICU admission scoring systems.
After a year of the pandemic, the most characteristic laboratory abnormalities for COVID-19 infection have already been defined. It has been confirmed that the pulmonary pathophysiology in severe COVID-19 infection is associated with a marked alveolar inflammatory cell infiltrate, together with a systemic cytokine storm response. Several studies have also reported evidence of a COVID-19-associated coagulopathy [26].
In our study, frailty was identified as an independent risk factors for death. Data from the literature indicate that in patients admitted to the hospital with COVID-19, disease outcomes were better predicted by frailty than either age or comorbidities [27]. This could be directly related to the fact that the second independent risk factor for death in our patients turned out to be low levels of total protein on admission. Data from the literature confirm the association between nutritional status and frailty syndrome in older adults, highlighting that malnutrition is an important determinant of this condition [28]. Although total protein level (containing 50–65% of albumin) is not considered a standard nutritional biomarker, it may indicate poor nutritional status caused by low protein intake before the onset of the disease or in the period preceding ICU admission.
In our study, 25% of patients had D-dimer levels above 5000 ng mL–1, but, interestingly, the proportion of such increased levels was similar in non-survivors and survivors (P = 0.851). In a retrospective study of 183 patients with COVID-19 infection, Tang et al. [29] observed that D-dimer levels assessed at hospital admission were higher in patients who did not survive hospital stay. The hypercoagulable state may be a cause of pulmonary microthrombosis and cerebral infarctions observed in critically ill patients with COVID-19 infection. Therefore, abnormal coagulation can be useful in predicting clinical outcomes and may serve as an independent biomarker for poor prognosis in these patients. It is possible, however, that this parameter may identify patients requiring ICU admission but may not accurately differentiate potential non-survivors from survivors among severely ill patients already requiring ICU treatment.
Procalcitonin (PCT) has emerged as a reliable biomarker of bacterial infection and can distinguish between bacterial and viral infections. Therefore, PCT levels may also be used to identify patients with COVID-19 and concomitant bacterial pneumonia [30]. Among our patients, 12.4% had PCT levels higher than 2.0 ng mL-l, which indicates that probably they already had bacterial coinfections at ICU admission. Moreover, ICU mortality among patients with admission PCT levels > 2 ng mL-1 was much higher and was identified as an independent risk factor for ICU death in a multivariable analysis. It has been previously observed that COVID-19 patients with elevated PCT levels had a more severe disease course and required ICU admission more often, but the absolute PCT values observed were not very high [30].
Another issue that should be discussed is the comparison of medications used in non-survivors and survivors during their ICU stay. Our results indicate that there were significantly more patients taking arechine/chloroquine, lopinavir/ritonavir and convalescent plasma among survivors (P = 0.027, 0.028 and 0.015, respectively). These results, however, may be prone to serious bias. The use of anti-viral drugs in our cohort was variable and based on the current recommendations of local specialists in infectious diseases extended to the whole study period. Importantly, no specific antiviral treatment for COVID-19 was recognised as safe and effective during the early phase of the enrolment period for our study [8]. Also, it has to be borne in mind that some medications might not have been available in the early stages of the pandemic, while others might have been used more in patients with a better prognosis. In a multivariable analysis, however, it turned out that the use (or lack of use) of any antiviral drugs was not an independent risk factor for death in our study group.
It has to be mentioned that a diverse group of various therapeutic agents has already been evaluated during almost two years of the pandemic. Among them, only remdesivir, dexamethasone, tocilizumab and baricitinib proved to be effective and therefore received recommendations of the Polish Agency for Health Technology Assessment and Tariff System (AOTMiT) for the treatment of COVID-19 [31]. Even though convalescent plasma received earlier recommendations of AOTMiT for the treatment of COVID-19, its use is not further supported by the current scientific results [32]. Additionally, the use of chloroquine, lopinavir/ritonavir, or amantadine is not supported by study evidence [31].
Evidence for a benefit of remdesivir in COVID-19 comes from two large randomised clinical trials. Regarding remdesivir, the ACCT-1 study conducted in over a thousand patients showed a shorter recovery time and a lower risk of death compared to the control group [32]. However, results of the open-label SOLIDARITY trial, conducted in over 5000 patients, did not confirm an advantage of remdesivir either in the entire population treated or in patients who required oxygen therapy [33]. The use of remdesivir for 5 days should be considered in patients with confirmed SARS-CoV-2 infection during the period of viral replication, i.e., not later than 5–7 days after the first symptoms of the disease, in patients with documented pneumonia and oxygen saturation of the peripheral blood ≤ 94% [31].
Almost all our patients were treated with steroids. The RECOVERY Collaborative Group confirmed that the use of dexamethasone resulted in lower 28-day mortality among patients receiving mechanical ventilation or oxygen at randomization, but not among those receiving no respiratory support [34]. This observation might be related to the “cytokine storm” associated with COVID-19 (causing acute respiratory distress syndrome with extensive alveolar injury), which is typical for severe COVID-19 and might be responsible for the fatal outcome of these patients. Undoubtedly, steroids are currently indicated in ICU patients with severe forms of COVID-19 infection; they were also used in virtually all patients in our study. Currently AOTMiT guidelines recommend the use of dexamethasone, at a dose of 6 mg per day, intravenously or orally for 7–10 days, in patients who require oxygen therapy or mechanical ventilation [31].
It should be noted that our study had several limitations. It is necessary to recognize that it was a retrospective, single-centre study. The sample size is relatively small (n = 113). Additionally, no details regarding ICU treatment were analysed in the study, including the circumstances and the causes of death. Moreover, patients referred for ICU admission were not compared with the remaining patients with COVID-19 treated in the other departments at the same time.
These limitations should be considered in the context of the pandemic situation – the data were collected when the country was struggling with the second and third waves of the pandemic. This might be a reason why generally there is still a lack of ICU data on COVID-19 patients in Poland.