







Introduction
Increase in numbers of cutaneous fungal infections is being observed around the world. Approximately nearly a billion people are estimated to have skin, nail or hair fungal infections [1, 2]. Dermatomycoses occur in every age group and can significantly decrease quality of life. Examining the prevalence and epidemiological trends of cutaneous fungal infections is necessary for developing new effective preventive, diagnostic and therapeutic methods. Many factors can influence the growth and patterns of global spread of the different species of fungi. In a constantly changing world it is nearly impossible to project the extent of an impact that global warming, overpopulation and extensive medication use will have on the prevalence of fungal disease.
Aim
This study was performed to investigate the differences between the prevalence of dermatophytes and cutaneous fungal infections observed at two mycological laboratories and their plausible causes.
Material and methods
Data from the Mycology Laboratory of the Department of Dermatology, Venereology and Allergology at the Medical University of Gdansk, Poland and Mycological Laboratory of the Department of Dermatovenereology at the State Medical University in Grodno, Belarus were collected from 1 January 2014 to 31 December 2016. During this period mycological examination was performed in 7324 patients in Gdansk, Poland and in 4729 patients in Grodno, Belarus who exhibited clinical signs and symptoms of cutaneous fungal infections. Samples were taken from affected epidermis, hair and nails which were used to make direct preparations in 20% KOH with 40% DMSO. Additionally cultures were prepared on modified Sabouraud agar, which were incubated for 6 weeks at room temperature. Positive cultures were examined based on morphological and microscopic features as well as biochemical tests were performed.
Results
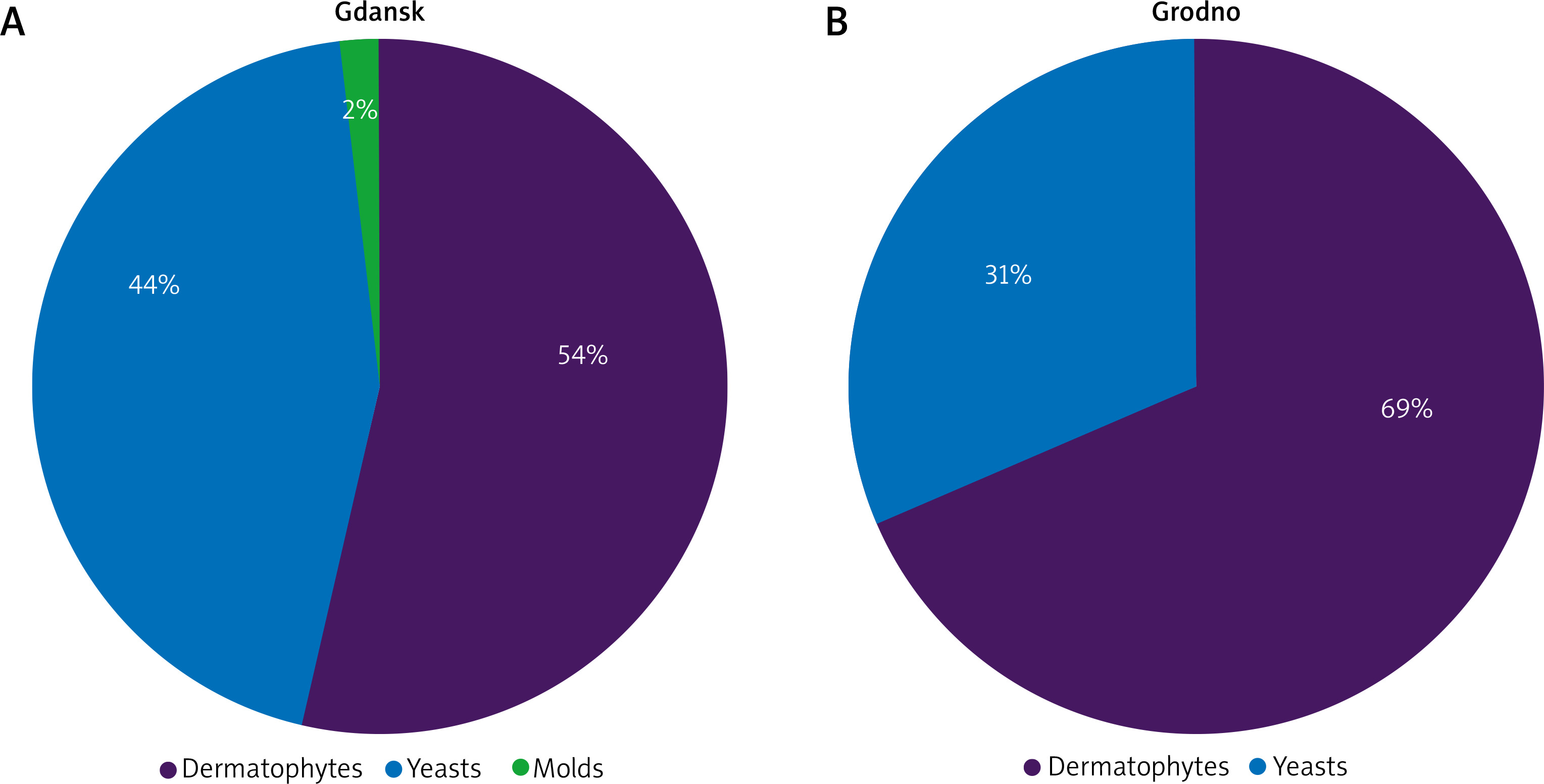
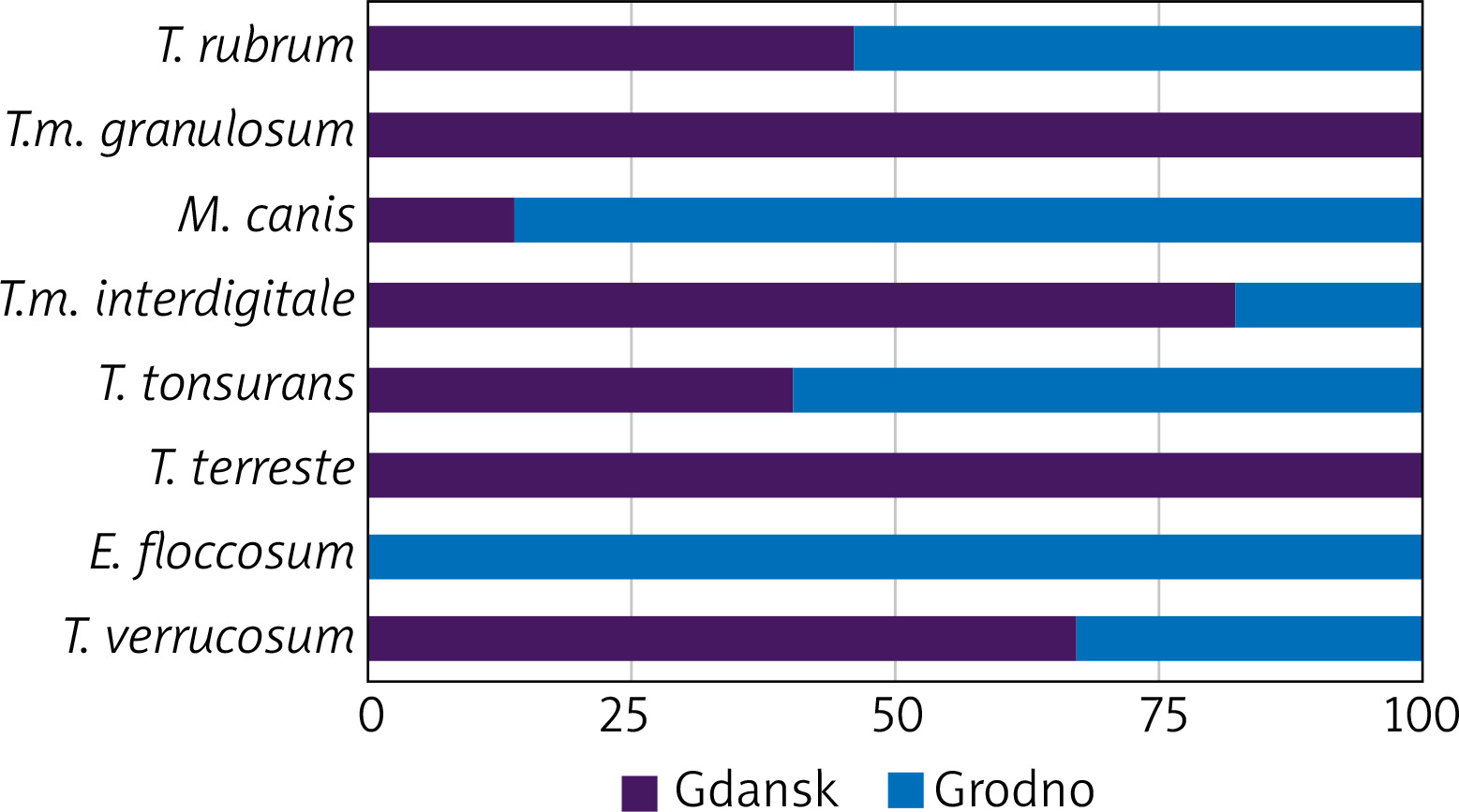
During the 3-year examination a total of 1196 confirmed cases of fungal infections were observed at the Mycological Laboratory in Gdansk. Dermatophytes were cultured in 642 (53.58%) cases. The most common species of dermatophytes were Trichophyton rubrum (306 cases), Trichophyton mentagrophytes var. granulosum (193 cases) and Microsporum canis (127 cases). Other species of dermatophytes such as Trichophyton mentagrophytes var. interdigitale, Trichophyton tonsurans, Trichophyton terrestre and Trichophyton verrucosum were isolated in less than 1% of the cases. Yeasts were isolated in 531 (44.40%) cases out of which Candida albicans was the most frequently identified in 323 cases. Additionally 28 mycologically confirmed cases of pityriasis versicolor (Figure 1) caused by Malassezia spp. were observed in Gdansk, Poland, what does not reflect the true prevalence of fungal infection. Due to a characteristic clinical appearance of pityriasis versicolor unfortunately in most cases this disease is treated empirically and mycological examination is performed in cases where the clinical picture is unambiguous. In order to conduct a systemic comparison between two laboratories a total number of Candida species will be compared due to the fact that the Laboratory in Grodno did not differentiate between different species of Candida. Moulds were cultured in 23 (1.97%) cases out of which Scopulariopsis brevicaulis caused 20 infections and Aspergillus spp. – only 3 cases.

During the same period of time 1685 cases of cutaneous fungal infections were diagnosed at the Mycological Laboratory in Grodno. Similarly, dermatophytes were the most common in 1158 (68.72%) cases. The vast majority of the superficial fungal infections were caused by Microsporum canis (788 cases) and Trichophyton rubrum (359 cases), other species Trichophyton mentagrophytes var. interdigitale, Trichophyton tonsurans, Trichophyton verrucosum and Epidermophyton floccosum were cultured in few cases. Candida were isolated in 527 (31.28%) cases. Also interestingly no cases of moulds were observed during that time period.
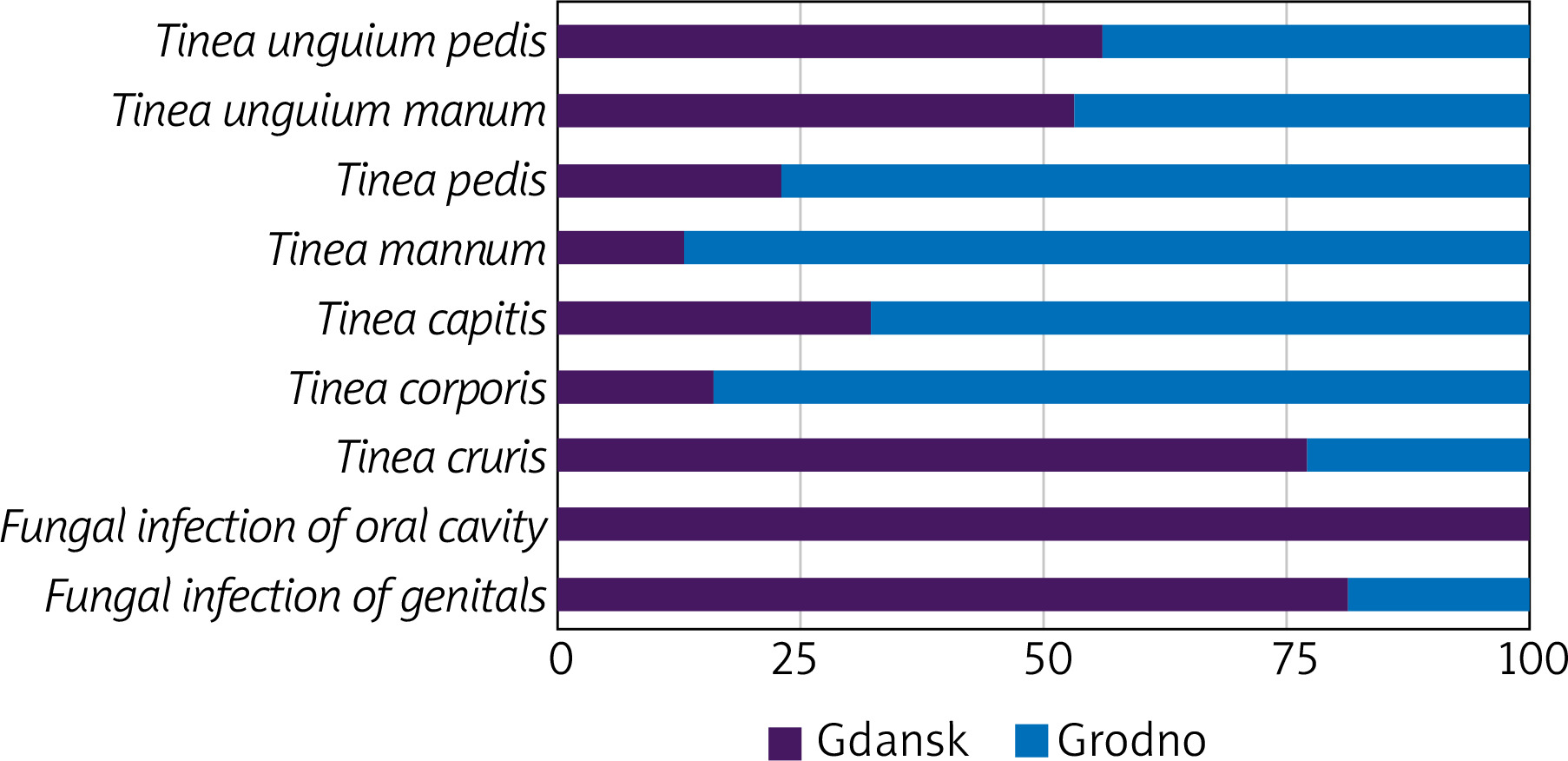
Analysing the localization of dermatomycoses onychomycosis was observed in majority of the infected patients in Gdansk. Mycological examination confirmed tinea unguium pedis in 534 patients, tinea unguium manuum in 295 patients followed by oral fungal infections and tinea corporis in 81 and 80 patients respectively. Other locations were involved in less than 10% of the cases.
In Grodno the most common location of superficial cutaneous infection was tinea corporis 547 confirmed cases followed by tinea unguium pedis (Figure 2) and tinea unguium manuum in 421 and 261 cases respectively. Tinea pedis, tinea capitis and tinea manuum (Figure 3) were diagnosed in nearly 10% of the cases each. Furthermore, tinea cruris and fungal infections of genitals were observed in single patients and no oral fungal infections were observed in the patients examined in the Mycological Laboratory in Grodno. Additionally, in the Gdansk region dermatomycoses were observed in 688 female patients and in 508 male patients. In Grodno the prevalence is inverted with the majority of cases observed in 921 males and 764 females.


The majority of the patients with mycologically confirmed fungal infection were over 16 years of age, namely 1092 cases in Gdansk and 1396 cases in Grodno. Fungal infections in both Gdansk and Grodno were predominantly observed in patients who live in the city with 1004 cases in Gdansk and 1021 cases in Grodno (Tables 1–4, Figures 4–6).
Table 1
Fungi observed in Gdansk (Poland) and Grodno (Belarus)
| Variable | Gdansk | Grodno |
|---|---|---|
| Dermatophytes | 642 | 1158 |
| Yeasts | 531 | 527 |
| Moulds | 23 | 0 |
Table 2
Species of fungi observed in Gdansk (Poland) and Grodno (Belarus)
Table 3
Localization of fungal infection
Discussion
Many factors such as environmental conditions, travel, and density of the population, culture, living conditions, and medication use and access to healthcare has an effect on dermatophytes and dermatophytoses of the region. Comparing the results of the superficial fungal infections of the two Mycological Laboratories can demonstrate the impact of different factors.
The two regions of the neighbouring countries that are separated by 400 km have similar environmental conditions with mean annual temperature of 8°C and average annual humidity around 80% except for the fact that Grodno experiences twice the annual amount of rainfall compared to Gdansk [3, 4]. This explains the reason why the numbers of confirmed cases of superficial fungal infections by Candida spp. and Trichophyton spp. are nearly the same, a substantial difference was observed in the number of Microsporum canis cases diagnosed which was the most frequent fungi cultured in Grodno.
On the contrary international travel can diversify fungal fauna, both foreign and returning travellers can affect the dermatophytes in the region, although dermatophytoses associated with travel are observed infrequently, constantly increasing international travel can increase the incidence of cutaneous fungal infections caused by rare or previously non-occurring dermatophytes in a given geographical area [5, 6]. In 2013 alone Poland was visited by 15.8 million tourists compared 137,000 visitors in Belarus, the result of this is the occurrence of fungi such Trichophyton terrestre which was observed for the first time in Australia in the 1950s or Trichophyton mentagrophytes var. granulosum which in the 1980s was the principal agent in the region of Valencia [7–10]. Moreover, direct variation was observed between higher population density and incidence of infectious diseases including superficial fungal infections [11]. The population density of the Pomeranian voivodeship is 130/km2 with a population of over 2,300,000 inhabitants compared to 43/km2 with a population of over 1,000,000 inhabitants. In both regions more than 1/3 of the population live in rural areas [12, 13]. Another important socioeconomic factor that has an influence on the ability of a patient to adhere and conclude the treatment plan is household disposable income per capita. In Poland the average pay is PLN 4517/month (EUR 1081) with a range of PLN 1008–4517 compared to BYN 850/month (EUR 345) with a range of BYN 0-995. When comparing minimal wages of two countries the difference is even more striking EUR 503/month compared to EUR 123/month respectively [14–16]. Furthermore according to a survey in 2001, the use of antibiotics in Poland was 22.5 defined daily doses per 1000 inhabitants compared to 8.0 in Belarus. This has a negative effect on microbiome and mycobiome which can lead to opportunist fungal infections [17]. The analysis of the results did not show this dependence once again showing that many factors contribute to prevalence of dermatomycoses. Lastly there is a significant difference in access to healthcare between the two countries, in Belarus on average there are 516 doctors per 100,000 inhabitants compared to 233 doctors in Poland [18, 19]. This difference can significantly decrease the waiting time for doctors’ appointments, which can hasten diagnosis and the onset of treatment, furthermore making a patient willing to seek doctor’s appointment.
Conclusions
The prevalence of superficial fungal infections is higher in Grodno, Belarus when compared to Gdansk, Poland. Similarly, dermatophytes were most commonly observed in both Laboratories. Analysing the factors that could influence, the prevalence of dermatomycoses showed that a lower socioeconomic situation and higher number of doctors available per capita resulted in the high prevalence and most likely diagnosis of superficial fungal infections.