





Dear Editor,
Clostridium difficile is a Gram-posi-tive, anaerobic, spore-forming bacillus commonly found in the environment, animals and people. C. difficile infection is one of the most common causes of infectious diarrhea [1]. Important risk factors of infection are broad spectrum antibiotics [2] especially second and third generation cephalosporins, clindamycin and fluoroquinolones [3]. The course of C. difficile infection might range from mild diarrhea to fulminant toxic megacolon [4]. The mortality of fulminant infection can be as high as 50% [5]. The effective method of treatment of recurrent and resistant C. difficile infection is fecal microbiota transplantation [6]. There are not many publications concerning this type of treatment in fulminant toxic megacolon [5, 7, 8]. There are also no data regarding proper patient preparation, method of administration and the timing of the treatment. We present a case of severe C. difficile infection treated successfully with fecal microbiota transplantation.
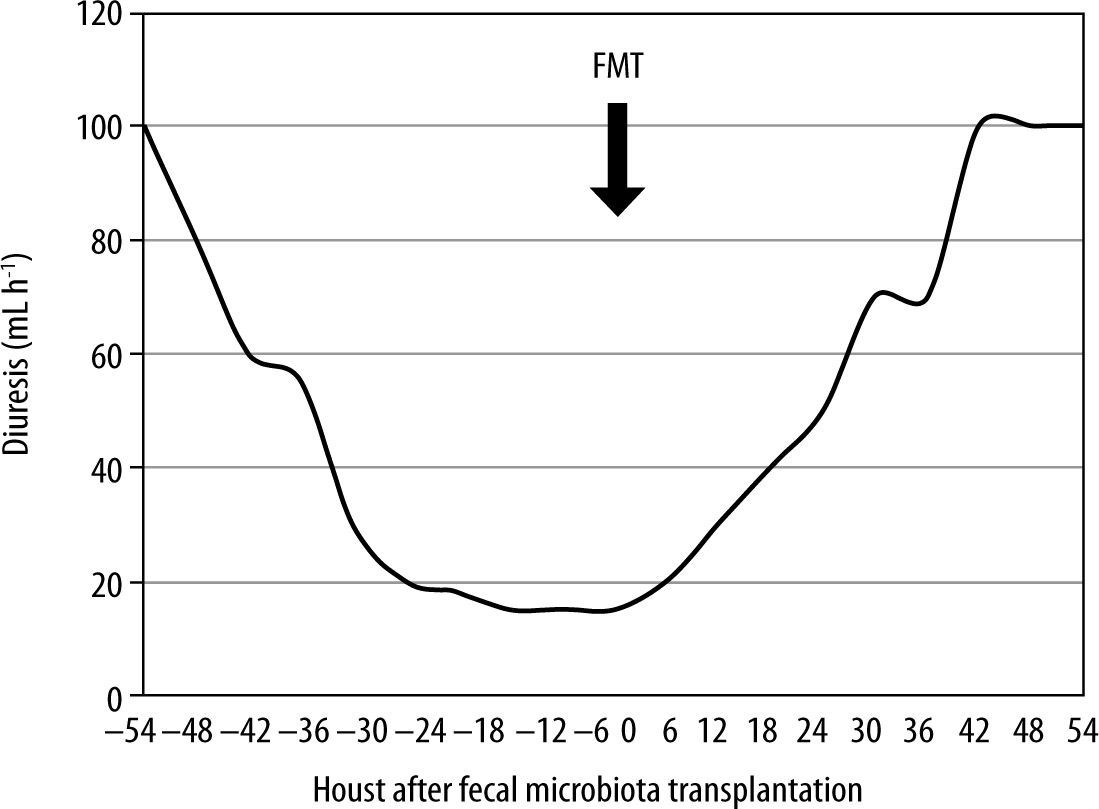
A 28-year-old man was admitted to hospital due to acute pancreatitis after alcohol abuse. The patient was given antibiotic treatment (amoxycillin/clavulanic acid) in the surgery department and after three days of hospitalization deteriorated due to systemic inflammatory response syndrome (SAPS II 21, SOFA 8) and was admitted to the ICU. The patient was started with noninvasive ventilation and supportive treatment. The antibiotic was stopped due to lack of signs and symptoms of systemic infection. Because the patient had diarrhea, C. difficile infection was suspected and confirmed with stool examination (positive toxin A and B). Antibiotics were given for severe infection (vancomycin 4 × 125 mg p.o. and metronidazole 3 × 500 mg i.v.). The patient remained in a severe condition mainly because of respiratory failure and paralytic ileus. CT scan of the abdomen showed severe intestinitis without pancreatic necrosis. Antibiotics were continued for 10 days and vancomycin 4 × 500 mg per rectum was started for complicated infection. Simultaneously supportive treatment was continued (mechanical ventilation, catecholamines, fluids and feeding). The patient improved (SOFA 2) and diarrhea stopped. After 7 days of antibiotic withdrawal, diarrhea reappeared and recurrent C. difficile infection was diagnosed. The antibiotics used in primary clostridium infection were introduced. After 4 days of renewed treatment the patient’s condition deteriorated, he developed fever, his neurology deteriorated as well as cardio-respiratory function (SOFA 9). Septic shock was diagnosed due to Escherichia coli infection with the point of origin in the intestine. Systemic antibiotics were introduced that led to quick progression of C. difficile infection. Paralytic ileus dominated in the clinical picture. CT scan of the abdomen showed toxic megacolon (Figure 1). Radical surgical intervention such as colectomy was considered, but eventually abandoned. The surgical team decided that the patient did not have any chance of survival and such a radical operation would not be beneficial. Emergency cecostomy was performed because of high intraabdominal pressure (IAP – 19 mm Hg) leading to acute renal failure requiring CRRT. After 10 days of ineffective treatment with antibiotics the patient was qualified for emergency fecal microbiota transplantation. We used unrelated donor fecal microbiota from a fecal microbiota transplantation (FMT) bank in the Medical University of Gdansk. In the course of preparation for transplantation vancomycin and metronidazole were stopped and systemic antibiotics for enteric sepsis were continued. It was difficult to decide which way to administer the prepared fecal microbiota. Administration through a nasogastric tube was virtually impossible due to gastroparesis, risk of regurgitation and ineffective transport through the pylorus. Colonoscopy was difficult to perform because the bowel could not be properly prepared and there was a risk of bowel perforation. We decided to inject 200 mL of prepared microbiota through cecostomy with a 100 mL syringe via a Foley catheter. Shortly after transplantation the patient still had fever, white blood cell count increased and the circumference of the abdomen increased due to bowel gas production. IAP transiently increased to 35 mm Hg and then started to decrease with subsequent peristalsis improvement. Normalization of IAP led to hemodynamic improvement (Figure 2) and return of adequate renal function (Figure 3). Two additional fecal microbiota transplantations were performed after 7 and 10 days. After every transplantation there was a transient inflammatory response with subsequent IAP reduction. After 65 days of ICU treatment the patient was transferred to a gastroenterology department.

FIGURE 2
Norepinephrine dose reduction as a result of hemodynamic improvement after fecal microbiota transplantation

C. difficile infection is a frequent cause of diarrhea in hospitalized patients. The clinical course can range from mild diarrhea to fulminant toxic megacolon. The fulminant form of infection is responsible for roughly 3% of all cases [9]. Fecal microbiota transplantation is a well-documented and recommended method of treatment in recurrent and resistant C. difficile infection [2, 10]. There are no guidelines and few data regarding this treatment in critically ill ICU patients [11–14]. We encountered a few problems in the presented case. Firstly we were unable to properly prepare the bowel for transplantation, which is highly recommended [2, 9] but virtually impossible in toxic megacolon. Secondly, we used systemic antibiotics for enteric sepsis, which might exacerbate C. difficile infection, as happened in the presented patient. We decided not to risk stopping antibiotics before fecal microbiota transplantation. Thirdly, we had a problem to decide on the best route of microbiota administration. We tried to choose potentially the most effective and safest access to the gastrointestinal tract. We decided to use cecostomy and administer microbiota through a Foley catheter introduced via cecostomy. Microbiota was prepared in a relatively large volume, which was meant to improve administration to deep parts of the intestine. There is still no credible evidence in the literature concerning the risk of fecal microbiota transplantation in critically ill ICU patients with toxic megacolon [5, 15]. After analyzing the indications [15, 16] we decided to perform FMT even without optimal patient preparation. The patient improved substantially after the first FMT, but after careful consideration we decided to perform 2 additional FMTs to increase the chance of permanent improvement. The procedure done in such suboptimal fashion proved to be safe for the patient. The inflammatory response observed after every FMT was transient as well as the increase in IAP. The presented case shows that fecal microbiota transplantation can be the treatment option for patients with severe C. difficile infection treated with systemic antibiotics in sepsis. We would like to point out that antibiotics used as prophylaxis for acute pancreatitis in the surgery department led to a severe case of C. difficile infection. The infection started only after four doses of amoxycillin/clavulanic acid. In spite of strong recommendations against using antibiotics in acute pancreatitis [17], such practice can still be found in some departments. The case presented shows that such practice can lead to more severe complications than primary pathology.