







Introduction
Anaphylaxis remains an important clinical issue in children.
Anaphylaxis is a clinical diagnosis, and it is based on identification of the characteristic symptoms that develop within minutes to a few hours following exposure to a known or potential trigger [1]. The widely used NAID/FAAN clinical criteria provide over 95% certainty in anaphylaxis diagnosis [2].
There are 23 known scales to determine severity of anaphylaxis [3], out of which Mueller’s scale is typically used to evaluate anaphylaxis following insect venom [4], Sampson’s scale for food-triggered anaphylaxis [5], Ring and Messmer’s scale is used to determine severity of anaphylaxis mostly in the German-speaking countries [6], as well as World Allergy Organization (WAO) scale and Brown’s scale originated from Australasia becomes more and more common [7]. Severity levels vary when evaluated with different scales, especially in case of anaphylaxis triggered by foods and medications [3]. Therefore, there is an increasing need for a homogenous methodology for diagnosis and classification of anaphylaxis, in particular in case of more severe symptoms [8]. A profile of the clinical symptoms may vary with age. There are only a few studies that evaluate this issue [9–11].
Aim
The aim of the study was to identify triggers of anaphylaxis and their influence on the clinical symptoms presented by the paediatric and adolescent patients treated in one of the tertiary paediatric centres in Poland, and to compare them to the European Anaphylaxis Registry data collected from the multiple paediatric centres. We are still working on the third report that will summarize diagnostic procedures employed to analyse the presented material.
Material and methods
Data regarding 126 children in the NORA Registry (Network of Severe Allergic Reactions) were derived from validated structured on-line questionnaires. That included each patient’s medical history and clinical evaluation of the symptoms in Ring and Messmer’s scale (R&M) upon admission for diagnostics and/or medical intervention due to an episode of anaphylaxis between September 2015 and March 2019. The Registry’s administrators confirmed and positively verified 114 questionnaires (90.5%). The study group included 114 children aged 5 months to 17 years (mean age: 8.0 ±4.8 years), with a male predominance (76 boys, 66%) in all age groups: 0–2 years (n = 17, 64.7%), 3–6 years (n = 32, 75%), 7–12 years (n = 40, 62.5%), ≥ 13 years (n = 25, 64%).
The parents or caregivers of the patients, and all the children older than 16 years signed voluntary informed consent forms to participate in the questionnaire study. The study was approved by the Ethics Committee of the Jagiellonian University (122.6120.250.2015). The work was supported by Jagiellonian University Medical College work funds (K/ZDS/006266). The presented study was a follow-up of a single-centre analysis, which was previously created in cooperation with the European Anaphylaxis Registry [12].
Statistical analysis
Qualitative data were presented as counts and percentages whereas quantitative data were given as means and standard deviations (SD). Between-group comparisons of qualitative variables were analysed by χ2 test; when expected frequencies in at least 20% of cells were lower than 5, the exact Fisher test was used for 2 × 2 tables and Fisher-Freeman-Halton χ2 test in the other cases. Comparisons of quantitative variables between two groups were conducted with the Student t test for independent samples. Differences between existence of subjective and objective symptoms in the same patients were estimated using McNemar test. The logistic regression model was used to evaluate the impact of age and elicitor on severity of the reaction. The results were presented as odds ratios along with respective 95% confidence intervals and respective p-values. A p-value of < 0.05 was considered significant. IBM SPSS Statistics 25 for Windows was used for statistical analysis.
Results
Almost all (99.1%) anaphylaxis incidents occurred in Poland, mostly at home (n = 43, 37.7%) or outdoors (n = 36, 31.6%).
The most frequent triggers of anaphylaxis were insect venom (n = 54, 47.4%), food (n = 40, 35.1%), drugs (n = 6, 5.3%), allergen immunotherapy (AIT) (n = 3, 2.6%), and other (n = 4, 3.5%). Idiopathic anaphylaxis (IA) was diagnosed in 7 (6.1%) children (Table 1). The elicitor classification was based on the NORA database. The type of allergens varied in different age groups (p = 0.016).
Table 1
Characteristics of the study group
In the group of children younger than 3 years (n = 17) and pre-schoolers aged 4–6 years (n = 32), food was the predominant anaphylaxis trigger, in 70.6% (n = 12) and 43.8% (n = 14), respectively. In the age groups of pre-teens, 7–12 year olds (n = 40) and teenagers (n = 25), the majority of anaphylactic reactions was caused by insect venom, in 65% (n = 26) and 52% (n = 13), respectively.
The types of food that triggered anaphylaxis included mostly animal products such as hen’s egg, cow’s milk, quail egg, fish, then tree nuts, spices, and fruits, followed by peanuts and other legumes (Table 2). The most common allergic foods in the children up to 3 years were hen’s egg (n = 6, 40%), cow’s milk proteins (n = 3, 20%), hazelnuts and sesame (n = 2 each, of 13.3%). In the 4–6 years age group, the most common food allergens included cow’s milk (n = 3, 27.3%), hen’s egg (n = 2, 18.2%) and single cases of hazelnuts, peanuts, cashews, linseeds, and kiwi (n = 1, 9.1%).
Table 2
Elicitors of anaphylaxis (n = number of cases)
In 2/3 of the cases, the food allergen was pre-packaged. In half of the cases, the food volume that caused the allergic reaction did not exceed 5 ml (1 teaspoon). Allergens in those cases were peanuts, hen’s egg, quail egg, tree nuts, and sesame.
The trigger in the majority of anaphylaxis cases caused by insect venom was a bee sting (Table 2). Children with venom allergy were older (mean: 9.2 ±3. years) than those with food allergy (mean: 5.9 ±4.9 years, p = 0.001).
Clinical manifestations of anaphylaxis typically included dermal (n = 113, 99.1%), gastro-intestinal (GI) (n = 70, 61.4%), respiratory (RS) (n = 107, 93.9%), and cardiovascular (CVS) (n = 85, 74.6%) symptoms (Table 1). The incidence of the symptoms from the gastrointestinal tract, respiratory system, or cardiovascular system varied depending whether children were allergic to insect venom or food (Table 1).
The cardiovascular symptoms developed in all the children in whom anaphylaxis was triggered by a drug, in over two thirds of patients allergic to insect venom, and in a smaller fraction of children with food allergy (p = 0.022). The GI symptoms were diagnosed in more than 3/4 of children with a drug or food allergy, and in less than half of those allergic to venom (p = 0.004) (Table 1).
Clinical characteristics of anaphylaxis varied when evaluated in four age groups (Figure 1 A). The children with GI symptoms were younger (mean: 7.16 ±4.5 years) than those without them (mean: 9.3 ±4.9 years, p = 0.019). The objective symptoms of anaphylaxis developed in all the patients (100%), while the subjective symptoms were experienced by 89.5% of children (p < 0.001). The objective symptoms included vomiting (p = 0.01), which dominated in the youngest patients aged 0–2 years (47.1%) followed by children aged 3–6 years (40.6%), and hypotension (p = 0.006) that was predominant in the 7–12 years age group (40%) (Figure 1 A).
Figure 1
Frequency of the listed anaphylaxis clinical symptoms as a function of the age group (A) or a specific trigger (B). A – the age groups included ages 0–2 (green column), 3–6 (red), 7–12 (blue) and 13+ (orange). B – the trigger was either insect venom (blue) or food ingestion (orange)
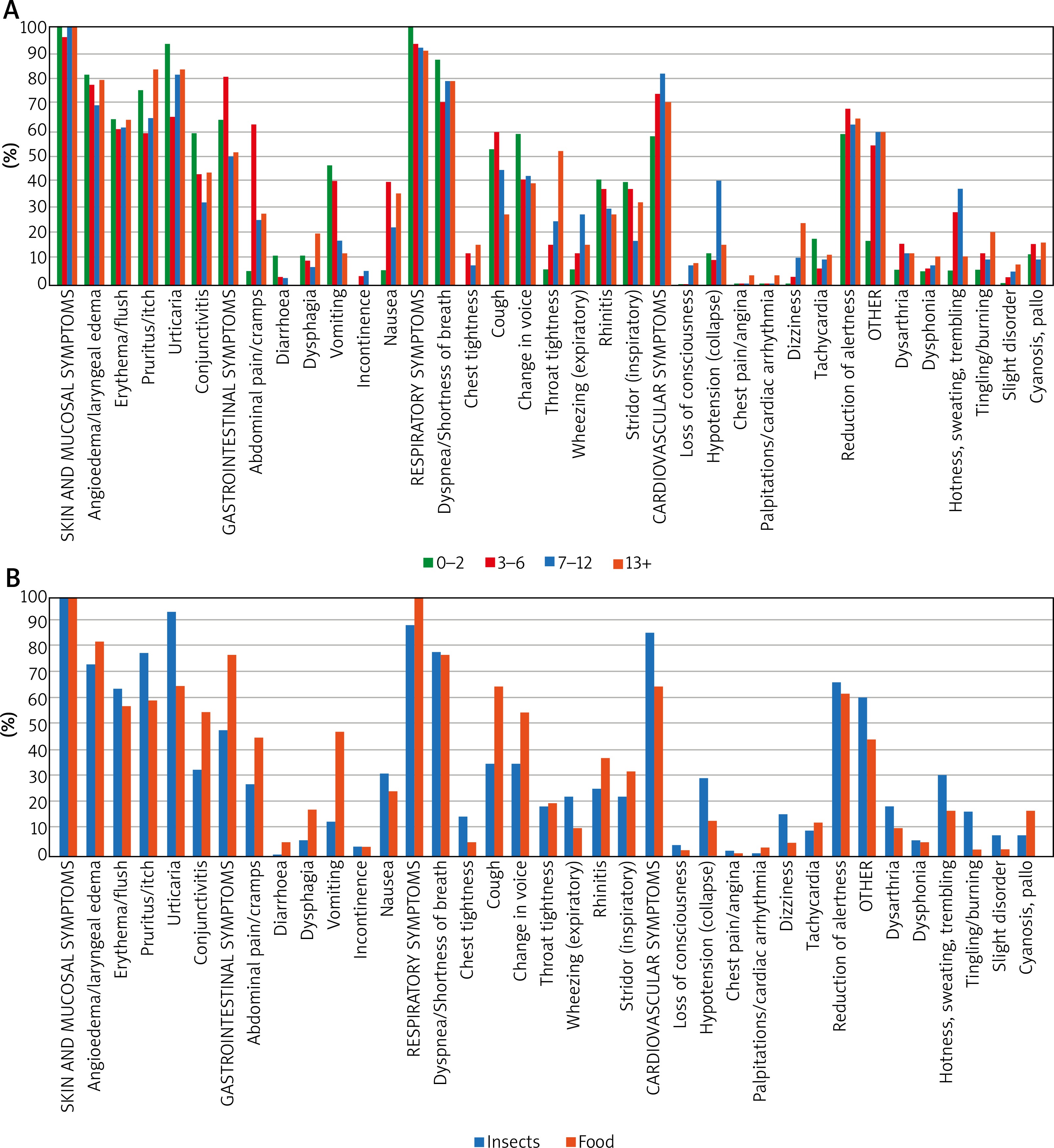
The subjective symptoms included abdominal pain (p < 0.001) and nausea (p = 0.044) that dominated in the 3–6 years age group, then throat tightness (p = 0.002) and dizziness (p = 0.022) in the 13+ years age group, and hotness, sweating, trembling (p = 0.027) in the 7–12 years age group (Figure 1 A). Food-triggered anaphylaxis was significantly more often associated with conjunctivitis (p = 0.036), vomiting (p < 0.001), and cough (p = 0.04) (Figure 1 B), while insect venom often resulted in tingling, burning of hands/feet (p = 0.04), paraesthesia, urticaria (p < 0.001), and hypotension (p = 0.049) (Figure 1 B).
Analysis of the symptoms’ severity showed grade IV in 85 (74.5%) children according to Mueller’s scale, and analogous grade III in 75 (65.8%) children according to the R&M scale. There were significant differences in their distribution when evaluated with either Mueller’s scale (grade II + III vs. IV; p = 0.028) or R&M scale (grade II vs. III; p = 0.029) between selected groups of the trigger factors. The most severe anaphylaxis cases were triggered by medications according to both scales (Figure 2 A).
Figure 2
Frequency of grade IV and grade III anaphylaxis as a function of different anaphylaxis triggers (A) or selected age groups (B)
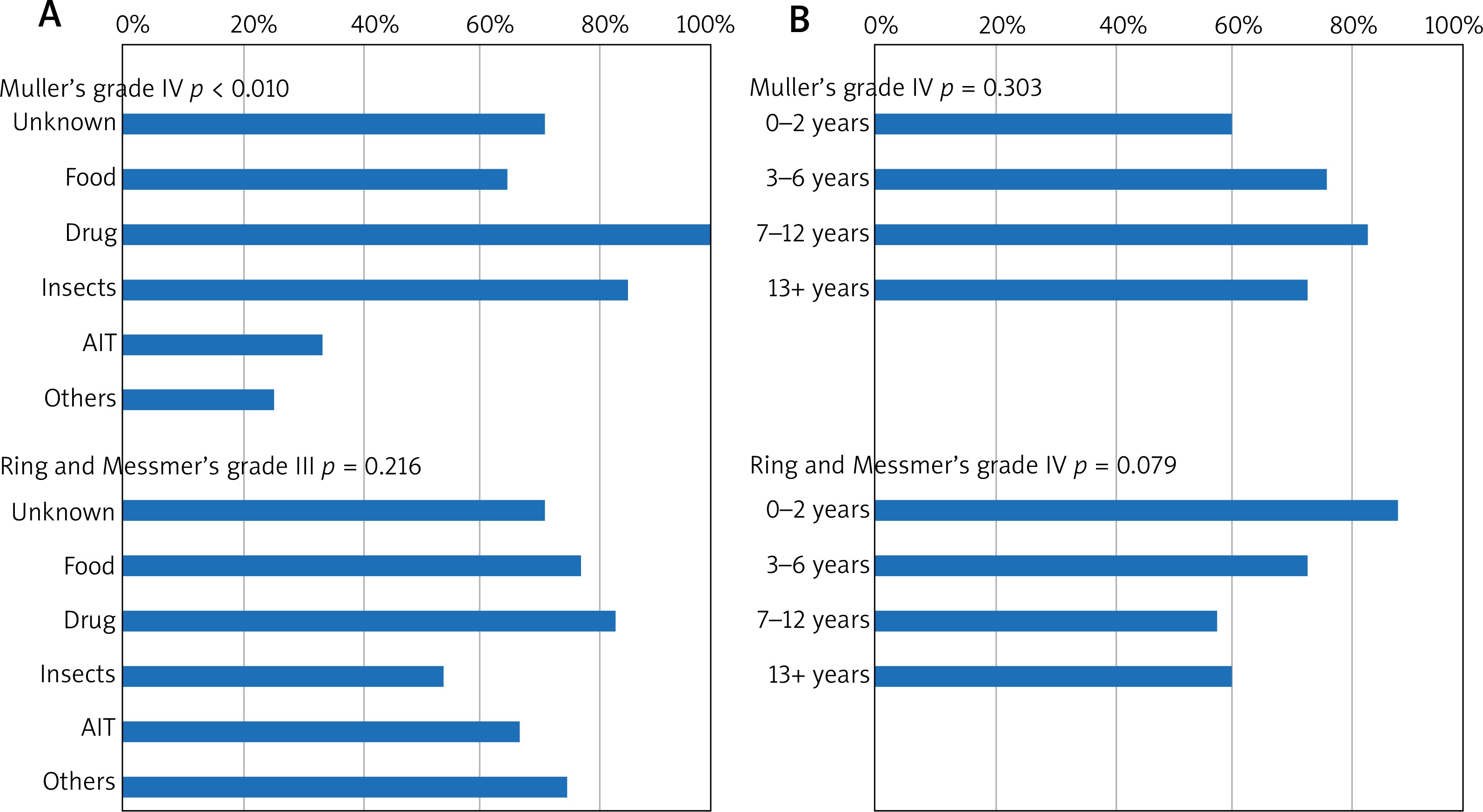
Mueller’s scale grade IV was most often diagnosed in anaphylaxis caused by medications and insect venom, while it was least common in AIT and other allergens. R&M’s grade III was the most common in the drug- and food-induced reactions, and the least common in the insect venom cases. The frequency of Mueller’s grade IV increased with age, and it was the most common in the 7–12 years age group, in contrast to frequency of R&M’s grade III.
Life-threatening symptoms were observed in 26 children (mean: 9.1 ±3.9 years) (14 boys), presenting as a blood pressure decrease (n = 25, 22%), and/or loss of consciousness (n = 5, 4.4%) (Table 3). The youngest children were the least susceptible to develop life-threatening reactions, which were observed in only 2 out of 17 children up to the age of 3 years (1.8%). The most common causative agents that triggered a severe life-threatening reaction were venoms (n = 17, 65.4%), food (n = 5, 19.2%), and drugs (n = 3, 11.5%). In 1 (3.8%) case, there was no causative agent found.
Table 3
Clinical presentation of children with potentially life-threatening anaphylaxis
In the group of 6 children allergic to medications, half of them developed a very serious case of anaphylaxis. Comparison of the frequencies of the life-threatening symptoms triggered by either food or insect sting showed that the symptoms manifested in every third child (31.5%) allergic to insect venom and every 8th patient (12.5%) allergic to food (p = 0.032).
In 110 out of 114 evaluated children (96%), we determined the length of time from the contact with the causal trigger to the first symptoms of anaphylactic shock. The above time period was less than or equal to 10 min in half of the above patients (n = 56/110, 50.9%). The shortest time (0–10 min) was observed in children exposed to AIT or unknown agent (66.7% in each of those groups), insect venom (57.4%), food (45%). The symptoms developed 30 min after the anaphylactic trigger’s exposure in 15.5% of children.
In the group of 6 patients that developed anaphylaxis after drug administration, the majority of them (n = 4, 66.7%) showed first symptoms after over 30 min. There was no age difference between the children who developed anaphylaxis quickly to the ones reacting after more than 30 min (p = 0.5). The time of development of the symptoms since the trigger exposure was not associated with the child’s gender (p = 0.85). The time of occurrence of the serious, potentially life-threatening symptoms such as loss of consciousness, hypotension, stridor, wheezing, throat swelling, was not different from the one of the milder symptoms (p = 0.774).
A biphasic reaction developed in 7% (n = 8) of patients in the 0–10 years age group due to allergy to food (fruit (1), hen’s egg (2), cow’s milk (2), bee venom (2), drug (paracetamol) and one unknown trigger, graded as grade III (all food allergens) and grade II according to R&M scale.
Multifactorial analysis
Grade IV according to Mueller’s scale was significantly less common (p = 0.028) in children who developed anaphylaxis triggered by the factors other than food and insects compared to the venom. There was no such a correlation found in case of R&M grade III. Age did not affect severity of the symptoms according to either scale.
Discussion
The issue of anaphylaxis in paediatrics remains important and it is characterized by the most dynamic increase compared to the other life-threatening conditions in children, though it varies according to the geographic region [13–15]. In the US between 2008 and 2014, there was a 147% increase of the reported anaphylaxis cases in children, from 101 to 249 million children per year [16]. The main reference system for our study was the European Registry of Anaphylaxis that included data of 1970 cases of children and adolescents [17]. The data from our centre constituted 12.5% of the international part of the Registry, compromising 909 cases of children and youth (https://www.anaphylaxie.net/en/#tabs-quote-1552943379-1744-1).
Age and place
The age distribution including 43% of 0–6 year olds, 35% of 7–12 year olds, and 22% of 13+ year olds, with a predominance of males (66.7%) in our study was comparable with the European Registry data (44%, 33%, and 23%, respectively) with the majority of boys (70%) [17]. The high proportion of males in anaphylaxis in children was recently presented in the meta-analysis based on 59 international paediatric publications [18]. A lower fraction of boys (58%) but a similar average age (7.4 ±4.7 years) compared to our work was presented by the French authors who analysed data of 160 children with anaphylaxis hospitalized in one of 18 paediatric emergency care units in the Nord-Pas-de-Calais region of France between 2015 and 2017 [19]. The majority of the presented anaphylaxis events occurred either at home (n = 43, 37.7%) or outdoors (n = 36, 31.6%), which was comparable with the European Registry data, 46% and 19% respectively [17].
Triggers
In the presented material, the most common anaphylaxis triggers were insect venom and food products. The most common food elicitors were hen’s egg, cow’s milk, sesame, peanuts and hazelnuts. Those allergens were predominant in the younger kids up to 3 years (70.6%) and pre-schoolers (43.8%). Both age distribution and type of allergens (triggers) were comparable with the Anaphylaxis Registry showing that food such as cow’s milk and hen’s egg caused 88% of reactions in children younger than 6 years, as well as other studies in the youngest children with anaphylaxis history [17–19]. An increasing number of paediatric reports indicated a growing role and strong allergic potential of the nuts, in particular tree nuts in the preschool children who developed allergic reactions to cashews and walnuts independent from their peanut or legumes allergy [20–22]. In our material, the tree nuts such as hazelnuts, walnuts, and cashews (n = 6) caused an anaphylactic reaction in children aged 0–10 years twice more often than peanuts. In the European Registry, anaphylaxis triggered by tree nuts was the most prevalent in the preschool children, 76% of children were allergic to cashews and 66% to hazelnuts in the group of 87 reported cases. At the same time, anaphylaxis due to peanuts was present in all the age groups, 325 cases out of the entire 1970 study’s cohort (16%) [17]. In this material, like in all the other centres, the majority of the anaphylactic reactions developed shortly after nut consumption, even in a small amount. In the majority of the paediatric studies, including anaphylaxis registry, the second most common trigger after food allergy is insect venom [17]. Stings by the wasp were predominant (n = 191 wasp stings vs. 161 bee stings) in the European Registry. Our study recorded the predominance of the children allergic to bee stings, since the majority of our patients were children of bee keepers. In contrast to the above observations, there was a recent French one-centre study from 2015–2017, in which insect venom was confirmed only in 1 case in a population of 152 children with anaphylaxis [19].
Also, in the French study, in contrast to our study (6.1%), more children (17%) developed IA where a trigger factor could not be identified [19]. French data were consistent with American studies, which in 2017 determined IA occurrence to be 17%, almost doubling from 10% recorded at the end of the 20thcentury [23]. IA was always a mark of system imperfection and limitation of diagnostic possibilities. Frequency of IA was not recorded in the European Registry.
Opposite to adults, in children confirmed drug-induced anaphylaxis occurs rarely. It is indicated both in our study as well as in the studies directly addressing the issue of drug allergy in children [24].
Symptoms evaluation
In our study, all anaphylaxis triggers caused dermatologic symptoms such as urticaria (79.8%), angioedema (76.3%), pruritus (69.3%), and erythema (61.4%). In the European Registry, the skin changes were recorded in 92% in the following order: urticaria (62%), pruritus (37%), and erythema (29%) [17].
The French authors reported similar observations, where the skin-associated symptoms developed in 99% of children with predominant rush, then pruritus, 1/3 had angioedema, 26% of children had OAS (this particular type of data was missing in the NORA questionnaire). It was surprising that there was no record of urticaria [19].
In our study, symptoms of the respiratory tract distress such as dyspnoea (78.9%), cough (46.5%), change in voice (43.9%), rhinitis (43.9%), stridor (29.8%), throat tightness (25.4%), and wheezing (17.5%) were observed in 93.9% of children. These were present in all the children (100%) with anaphylaxis induced by medication, AIT and other allergens. In the European Registry, 80% of children developed respiratory system distress in the form of dyspnoea occurring with the same frequency in all the age groups, and about 1/3 of children suffered from wheezing [17]. In the French study, only 64% of children experienced respiratory problems, including dyspnoea that developed in 56%, stridor in 19%, in none of them there was any bronchial obstruction, but they were present in 18% of children in the ambulatory care and ED [19].
Our data indicated that 61.4% of children manifested GI symptoms, with a significant difference between children with food allergy (77.5%) and the ones allergic to insect venom (48.1%). Abdominal pain was the most common GI symptom, however only vomiting was significantly predominant in the children with food allergy (48%) compared to the insect venom (13%) in particular in the 0-6 years age group. Similarly, the Registry data indicated GI symptoms in 45% of cases with predominant vomiting in the preschool group (27%) and nausea in the school children (15%) [17]. In the French study, less children developed GI symptoms (48%), out of whom the majority reported abdominal pain (36%) and vomiting (30%) [19].
In this study, the cardiovascular (CV) symptoms were present in 74.6% of children. They were significantly more common in the children allergic to insect venom (85.2%) compared to the food products (65%), and they occurred in all the children with drug-induced anaphylaxis. The Registry recorded CV symptoms in 41% of cases, mostly in the form of dizziness, hypotension and collapse, more prevalent in the adolescents [17]. In the French study, the CV and neurological symptoms were combined and recorded as a loss of consciousness in 13% of children, and documented hypotension at the level of ED in 3% of patients [19]. Three percent of the French parents reported altered consciousness (reduction of alertness) of their children [19]. In our study, the parents noticed an altered mental state in 64% of children, including all the patients allergic to medications and 67% of them allergic to insect venom. In the Registry, 13% of children experienced a decreased level of consciousness [17].
There is no universal tool to assess severity of anaphylaxis across the entire spectrum of symptoms, variety of age groups, different potential triggers and exposure circumstances. There is a number of heterogeneous scales out of which some are dedicated to a specific type of antigen that triggers anaphylaxis. All those instruments typically evaluate milder, not life-threatening symptoms, such as urticaria, however they might over- or underestimate more severe clinical symptoms [3]. Therefore, there are discrepancies in the severity assessment with different scales, which was further demonstrated by the multifactorial analysis in this study. According to the Registry, the majority of the anaphylactic reactions evaluated with R&M’s scale were grade III (47%, 2 organ systems seriously affected) and grade II (45%, ≥ 2 organ systems affected); anaphylaxis was instantaneous within 10 min from the trigger exposure in 58% of children, and it was biphasic in 5% of children (n = 77) [17].
Our data were different since 62% of children developed grade III reaction and 37.7% of them had grade II according to R&M’s scale. However, the observed timeline of the events was comparable, where about half of the patients developed anaphylaxis within 10 min, and 7% had a biphasic type of reaction.
In the Registry there were 26 (1.3%) cases with potentially life-threatening reactions in all the age groups, including 7 cases of cardiac failure and 5 deaths caused by cow’s milk, peanuts, and insect venom [17]. In our material, we did not record any deaths, however 26 (22.8%) children developed potentially life-threatening symptoms as a result of anaphylaxis to insect venom (n = 16), foods (n = 5) and drugs (n = 3).
We identified 36 (31.6%) children who developed anaphylaxis after repeated exposure to the same allergen as before. The Registry reported a comparable number of about 1/3 of children experiencing anaphylaxis in the past [17]. According to the French study on the recurrence of anaphylaxis in children hospitalized at PICU in 2003–2013, the recurrence rate of anaphylaxis was 0.20/100 patients/year, while food (79%) and drugs (8%) were the main elicitors [25].
Symptomatology vs. trigger of anaphylaxis
The differences in symptoms that varied depending on the type of the anaphylaxis trigger were also noticed by Danish researchers [3]. Their study included all the patients with the positive results of food or drug provocation tests (n = 2828), including 616 cases of anaphylaxis. The most frequently recorded symptoms following food challenge were urticaria (47%), oral allergy syndrome (OAS) (35%), abdominal pain (32%), conjunctivitis (24%), vomiting (24%) and rhinorrhoea (22%), while drug-induced anaphylaxis was characterized predominantly by the skin symptoms such as pruritus (47%), urticaria (36%), rash (35%) or angioedema (17%) [3]. The patients undergoing food challenge were significantly younger than these challenged with a drug (p < 0.001). The Danish authors pointed out that the youngest children in the 0–3 years group rarely had subjective symptoms, such as OAS, abdominal pain or nausea, instead more of them (63%) had urticaria and/or rhino-conjunctivitis, compared to the older age groups (4–15 years/15+ years). The 15+ years group presented more severe objective reactions after a challenge with peanuts (a-OR (95% CI): 1.77 (1.33–2.35)), while other food challenges in this group were significantly milder (p = 0.03), especially when compared to drug challenge outcomes [3]. Nevertheless, it appeared that there was a number of underdiagnosed cases of severe anaphylaxis in the youngest group of patients, in whom food was the most common causative factor. In our material, up to 80% of children aged 0–3 years demonstrated R&M’s grade III anaphylaxis. In the French study based on anaphylaxis cases recorded by the Allergy Vigilance Network from 2002 to 2018, it is pointed out that hypotension in young children (0–2 years) might be underdiagnosed [22]. According to their data, hypotension occurred in 21% of infants, which was significantly more frequent in comparison to preschool children (p = 0.004) [22]. Regardless of the age, all the children should undergo objective evaluation of their symptoms, including monitoring of blood pressure, heart rate, capillary refill time, and saturation if possible in order not to overlook any of these symptoms [26, 27].
The French authors carried out a detailed comparison of the symptoms resulting from antibiotics versus NSAIDs in children [3]. Our study included mostly children allergic to insect venom or foods; therefore we analysed those two groups. We observed that the children allergic to food were younger. Both groups almost always developed symptoms affecting their skin and mucous membranes.
In case of food-induced anaphylaxis, the GI tract (77.5% vs. 48.1%, p = 0.004) and respiratory tract (100% vs. 88.9%, p = 0.036) associated symptoms were significantly more common compared to the insect venom. In contrast, anaphylaxis resulting from insect venom mostly affected the CV system (85.2% vs. 65%, p = 0.022).
It is suggested that similarly to asthma, we may expect some differences between anaphylaxis caused by food vs. non-food triggers, with respect to different anaphylaxis endotypes, based on different pathophysiological patterns, which may vary in clinical manifestations [28].
This is a retrospective study. Additionally, our department serves as the reference centre for diagnostics and treatment of insect venom-induced anaphylaxis in Southern Poland. We could not verify our data with respect to bias since there were no other extensive epidemiological studies of anaphylaxis triggers in children in Poland [29].
Conclusions
Clinical manifestations of anaphylaxis in children are both trigger and age dependent. Dermal and respiratory symptoms are present in almost all children. The phenotype of the patient with food anaphylaxis presents as a younger child with mostly GI symptoms, while the phenotype of the patient with venom anaphylaxis presents as an older child with mostly cardiovascular symptoms. Evaluation of the objective symptoms should be obligatory in all age groups.