









Introduction
A pro-health lifestyle, including recreational physical activity, is key in creating and strengthening health potential, preventing chronic diseases, and delaying involutionary changes. Physical activity with the characteristics of health training, including endurance and resistance as well as balance, mobility, and flexibility exercises, has a positive influence on holistically defined health in the biological and psychosocial dimensions of older people, including body composition, physical fitness, functional fitness, cognitive functions, social integration, mental well-being, and satisfaction with life [1–7]. Physical activity is of particular significance during aging because the changes typical of this period, related to, among others, a decrease in muscle mass, physical capacity, and functional efficiency, contribute to the deterioration of the quality of life [3, 7–10].
Despite the key importance of behavioural factors for health and quality of life, in numerous studies, a low level of physical activity among seniors in various countries has been indicated [11–15], further reduced during the COVID-19 pandemic [16]. In this context, an important role in public health policy should be played by the promotion of a healthy lifestyle, including recreational physical activity. Due to the aging of societies, health promotion programmes for seniors are becoming particularly important, as pointed out by numerous authors, i.e. from Scandinavia [17], Taiwan [18], the Netherlands, Germany, Italy, and Poland [19]. In this area, the Active Healthy Senior project was implemented in Kraków (Poland) between 2019–2022. The aim of the programme was to improve the psychophysical fitness of older people through participation in recreational activities (health training) and lectures on modified conditions of the aging process and the possibility of delaying involutionary changes. The programme was implemented in 2 editions, each lasting 9 months, during which seniors participated in various forms of physical activity, including Nordic walking, smovey®, psychophysical exercises (BodyArt), and aqua aerobics. The exercises took place twice a week, for 90 minutes (a total of 180 minutes per week).
Therefore, in relation to the nature of the psychophysical activation classes conducted for seniors from the Kraków community, research was carried out to compare the values of body mass index (BMI), functional fitness, satisfaction with life, and quality of life among senior women before and after the completion of the health training programme implemented during the 9-month period as part of the Active Healthy Senior project. In this context, the aim of the research was to evaluate the programme in terms of its importance for somatic index, functional efficiency and quality as well as satisfaction with life. The research hypothesis was adopted that active participation in a health training programme over a period of 9 months influenced the change in the analysed variables, including a decrease in BMI, an increase in the level of functional fitness as well as an increase in satisfaction and quality of life among senior women.
Material and methods
Participants
The research was conducted twice, among women who participated in the second edition of the Active Healthy Senior project, implemented at the University of Physical Education in Kraków (POWR.03.01.00-00-T225/18) as part of the Knowledge Education Development for the 2014–2020 EU operational programme. Information about the planned programme was posted on the University of Physical Education website and disseminated by the representative of the Mayor of the City of Kraków for seniors. Access to the programme was open to people aged 60+. Recruitment was purposeful and took place through voluntary application of people interested in response to a public announcement about the planned Active Healthy Senior programme. The applicable criteria were age 60+, declaration of availability to regularly participate in activities throughout the entire project period (9 months) and declaration of good general health allowing participation in recreational physical activity (twice a week for 90 minutes).
The first test (pre-test) was conducted at the beginning of the programme in September 2021, and the second test (post-test) in June 2022, after 9 months of participation in the health training programme. During this period, women participated in 3 physical activity modules, selected from Nordic walking, smovey®, BodyArt, and aqua aerobics. The exercises took place regularly twice a week, and a single training session lasted 90 minutes (i.e. 180 minutes per week). The health training was planned with reference to the World Health Organisation (WHO) 2020 guidelines on physical activity and sedentary behaviour of adults and older adults [1]. Physical exercise and tests were carried out at the University facilities by the authors of the work, specialists in the field of health training, physical fitness, nutrition, and nutritional status, as well as psychology. The research study was performed in accordance with the 1975 (revised in 2000) Declaration of Helsinki, after obtaining the participants’ written informed consent, while the research protocol was approved by the Bioethics Committee of the District Medical Chamber in Kraków (No. 166/KBL/OIL/2018).
The study included a group of 74 women aged 60–83 years, the mean age being 67.8 (±5.1) years. The group consisted of all program participants for whom complete data were collected. The group size, assessed in the G*Power program, for repeated measurement and a significance threshold of 0.05 was 64 people for a strong effect. The socio-demographic characteristics indicate that the sample was dominated by women living in Kraków (87.8%), with higher (55.4%) and secondary education (39.2%), declaring an average financial situation (78.4%) (Table 1). Assessing their health condition, the women declared the occurrence of chronic diseases, including hypertension (32.4%), osteoporosis (14.5%), type 2 diabetes (10.8%), irritable bowel syndrome (8.1%), and gout (5.4%).
Table 1
Socio-demographic characteristics of group (N = 74)
Instruments
Body mass index evaluation
Body height and body mass were measured to the nearest 0.1 cm and 0.1 kg with a portable SECA model 764 device (SECA, Hamburg, Germany). Measurements were obtained based on the following formula: BMI = body mass (kg)/height (m2). Anthropometric measurements were performed in the morning, and the participants were previously informed about how to prepare for the tests (on an empty stomach, after urination and bowel movement). In accordance with WHO recommendations, in the interpretation of BMI, for women below the age of 65 years, the range of 18.5–24.9 kg/m2 was adopted as the normative value, while for women aged 65+ years, the range of 22–27 kg/m2 was assumed as the desired body mass.
Functional fitness evaluation
Physical fitness was assessed using the functional fitness test (Senior fitness test, Fullerton functional fitness test). The test consists of 6 fitness tests, including: 1) 30-second arm curl test (evaluating upper limb muscle strength); 2) Back scratch test, the so-called safety pin test (assessing upper limb flexibility); 3) 30-second chair stand test (assessing pelvic and lower limb muscle strength); 4) Chair sit-and-reach test (gauging lower body flexibility); 5) 2.44-m up-and-go test (measuring agility and dynamic balance); 6) Two-minute step-in-place test (assessing endurance and exercise tolerance) [20]. Functional fitness measurements were carried out in accordance with standards determining their proper conduct, i.e. after a warm-up, including stretching exercises.
Evaluation of quality of life and satisfaction with life
The quality of life was assessed using the World Health Organization Quality of Life questionnaire (WHOQoL) in the Polish adaptation by Wołowicka et al. [21]. The scale is used to assess the quality of life among healthy and ill people (for cognitive and clinical purposes). It contains 26 questions enabling the assessment of the quality of life profile in terms of 4 dimensions of life: somatic (physical), psychological, social, and environmental. The results are presented as transformed in accordance with the WHOQoL-100 version and WHO recommendations.
Satisfaction with life was assessed using the satisfaction with life scale (SWLS) in the Polish adaptation by Juczyński [22]. The results of the SWLS consist of 5 items with a range of 5–35 points, and the higher the score, the higher the level of satisfaction with life. The reliability index of the Polish version of the SWLS according to Cronbach’s α is 0.81 [22].
Statistical analysis
Calculations were performed using Statistica 13.1. Basic descriptive statistics are presented (mean, median, standard deviation, minimum, maximum, lower, and upper quartiles). To determine the relationships between variables, Pearson’s correlation coefficient analysis (for pairs of variables with normal distribution) and Spearman’s correlation analysis (for pairs of variables in which at least one had non-normal distribution) were used. Student’s t-test for dependent measurements (in the case of variables with normal distribution) and the Wilcoxon paired test (in the case of variables with non-normal distribution) were applied to establish differences in BMI, SWLS, and functional fitness indices between the first and second measurements. The distribution of BMI in age categories was compared using the χ2 test. To determine the dependence of the quality of life profile on measurements, interactive repeated measures analysis of variance (general linear models) was used, along with planned comparisons and contrasts. The assumed significance level was α = 0.05. In the case of the back scratch variable, the distribution was significantly different from normal; therefore, the median was selected as a measure of central tendency.
Results
Descriptive statistics of analysed variables
The average BMI values for 2 measurements were 27.43 vs. 26.75 kg/m2, respectively. Taking the age criterion into account, women below 65 years of age obtained the following BMI results in subsequent measurements: 28.26 vs. 27.04 kg/m2, and older women: 27.47 vs. 26.40 kg/m2, respectively. In the area of functional efficiency (Fullerton test), in subsequent measurements, the average number of repetitions for the 30-second chair stand test was 15.86 vs. 18.18, and for the arm curl test, 17.16 vs. 19.07, respectively. In the chair sit-and-reach test, the results were 8.70 vs. 7.66 cm, for the up-and-go test, the results were 4.94 vs. 4.97 seconds, and for the 2-minute step-in-place test, they totalled 105.70 vs. 111.85 steps, respectively. The mean values of satisfaction with life (on the SWLS) were 24.43 and 25.36, respectively, meaning a slightly satisfying level. The level of quality of life (WHO scale) in subsequent measurements was, in the somatic area: 12.97 vs. 13.41, psychological: 14.02 vs. 15.55, social: 14.79 vs. 14.52, and in the environmental sphere: 14.82 vs. 15.38, respectively (Table 2).
Table 2
Descriptive statistics of analysed variables for 2 measurements (before and after 9-month pro-health training programme) (N = 74)
Changes in body mass index, functional fitness, and level of satisfaction with life
Comparison of the analysed variables demonstrated significant changes in BMI value and the level of functional fitness between the first and second measurements (Table 3). It was found that the average BMI value decreased (p < 0.001), while the functional fitness indices, including the 30-second chair stand (p < 0.001), 30-second arm curl (p < 0.001), back scratch (p = 0.001), and two-minute step-in-place (p = 0.002), increased. The level of satisfaction with life increased slightly between measurements, but this change did not reach the level of statistical significance (p > 0.05).
Table 3
Body mass index, functional fitness, and satisfaction with life as well as quality of life among women (before and after 9-month pro-health training programme) (N = 74)
In the first measurement, there were no statistically significant differences in the number of overweight, obese and normal weight women depending on age (χ2 = 5.29; p = 0.071), while for the second measurement, the difference was statistically significant (χ2 = 9.48; p = 0.010). Moreover, 29.2% of women below the age of 65 and 64% of women above 65 years of age had normal BMI. In turn, obesity (BMI ≥ 30 kg/m2) was observed in 29.2% of women from the younger age group and 22% from the older one (Table 4).
Table 4
Distribution of body mass index among women depending on age (below and above 65) before and after the implementation of the health training programme (percentages of respondents, χ2 test)
Changes in particular aspects of quality of life
The quality of life profiles between the first and second measurements showed significant differences (p < 0.001) (Table 5). A change was demonstrated both between the first and second measurements, as well as in the quality of life profiles in both measurements (Fig. 1).
Table 5
Profile of quality of life among women (measurements before and after 9-month pro-health training programme) (N = 74)
| Parameters | df | F | p-value | Partial η2 |
|---|---|---|---|---|
| Intercept | 1 | 8909.54 | < 0.001 | 0.99 |
| Error | 73 | |||
| Measurement | 1 | 15.16 | < 0.001 | 0.17 |
| Error | 73 | |||
| WHOQoL | 3 | 62.47 | < 0.001 | 0.46 |
| Error | 219 | |||
| Measurement WHOQoL | 3 | 23.53 | < 0.001 | 0.24 |
| Error | 219 |
Fig. 1
Profiles of quality of life among women in consecutive measurements (before and after 9-month pro-health training programme)
1 – somatic aspect, 2 – psychological aspect, 3 – social aspect, WHOQoL – the World Health Organization Quality of Life 4 – environmental aspect
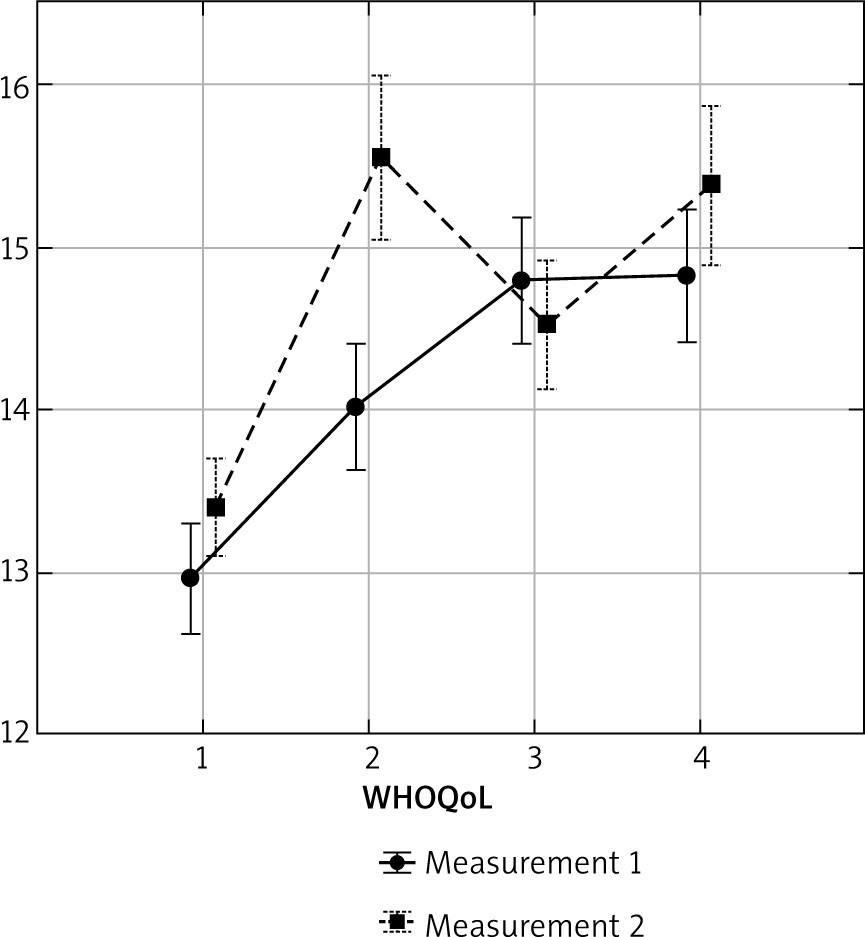
Between the first and second measurements, three aspects of quality of life (somatic, psychological and environmental) intensified, with the greatest increase recorded for the psychological aspect (Table 6).
Table 6
Selected aspects of quality of life among women (before and after the 9-month pro-health training programme) (pre-test vs. post-test, N = 74)
| WHOQoL | Mean1 | SD1 | Mean2 | SD2 | F (1.73) | p-value |
|---|---|---|---|---|---|---|
| Somatic | 12.97 | 1.47 | 13.41 | 1.29 | 7.33 | 0.008 |
| Psychological | 14.02 | 1.66 | 15.55 | 2.19 | 45.87 | < 0.001 |
| Social | 14.79 | 1.68 | 14.52 | 1.70 | 1.63 | 0.205 |
| Environmental | 14.82 | 1.76 | 15.38 | 2.11 | 9.71 | 0.003 |
There were also differences in the quality of life profiles in the first and second measurements (Table 7). In the first one, the somatic aspect of quality of life achieved the lowest level, while the social and environmental aspects were rated the highest. In the second measurement (after 9 months of pro-health training), the somatic aspect was still the lowest, but this time, women rated the psychological and environmental aspects the highest. The environmental aspect was rated higher than the social aspect.
Table 7
Comparison – profiles of quality of life among women for the first and second measurements
Discussion
In the present research under discussion, statistically significant positive changes have been shown in BMI and the level of functional fitness as well as quality of life after 9 months of women’s active participation in the health training programme (Nordic walking, smovey®, BodyArt, aqua aerobics). Despite the positive trend, there was no significant change in satisfaction with life, thus, the accepted research hypothesis about the positive impact of health training on the analysed variables was partially positively verified. The obtained results generally confirmed the positive impact of systematic recreational physical activity with the characteristics of health training on various indicators of holistically defined health and quality of life of women above the age of 60.
Discussing the analysed variables one-by-one, it should be noted that women 60+ participating in the health promotion programme had an above-average BMI value (exceeding 25 kg/m2, therefore, these values were in the overweight range according to WHO). Considering the age criterion, it should be clarified that the mean BMI values for women below the age of 65 were in the overweight range (above 25 kg/m2), while older women (65+) were in the upper limit of so-called desired body mass (approximately 27 kg/m2). The level of BMI was similar to the values obtained in other groups of older women, including those participating in the first edition of the Active Healthy Senior project, for whom this value was 27.3 kg/m2 [23], as well as among women aged 50–86 from an American population including various ethnic groups, in whom this level was 26.6 kg/m2 [24]. Lower BMI values, at the level of 23.7 kg/m2, were described among women aged 60–75 from Switzerland and France [25]. Increased BMI values increase risks for health [26].
Assessing the level of the analysed fitness variables in the studied group of women 60+ (regardless of the measurement) showed a level of functional fitness indicators allowing for independent functioning, with the initial results (pre-test) being similar to those obtained among women participating in the first edition of the programme (at the beginning implementation), especially for the 30-second chair stand (15.4 repetitions) and the 2.44-m up-and-go (4.8 sec) tests [23]. Studies conducted among the Chinese population showed differences in the level of functional fitness of seniors depending on gender, with an indication of a higher level of flexibility in women [27].
In terms of the level of satisfaction with and quality of life, results were also obtained similar to those achieved among women participating in the first edition of the Active Healthy Senior programme [23, 28]. Women who signed up for the health promotion project demonstrated an average level of satisfaction with life, which is a subjective measure of quality of life. In other Polish studies, a similar, average level of life satisfaction was shown, including among women with type 2 diabetes [29]. In terms of quality of life according to WHO, the surveyed women (in both measurements) rated the physical (somatic) aspect of quality of life the lowest, similarly to women participating in the first edition of the programme [28].
Referring to the aim of the study, it should be stated that the discussed research allowed to indicate a statistically significant decrease in all 60+ women’s BMI after 9 months of implementing the health training programme (27.4 vs. 26.7 kg/m2). It was also found that during the health training period, the maximum BMI value in the group decreased (43.2 vs. 37.8 kg/m2), which means that after implementing the programme, there were no morbidly obese women among the respondents (i.e. above 40 kg/m2). Taking the age criterion into account, it should be noted that the decrease in BMI concerned both women below and above the age of 65, while in older women, it was accordance with the so-called desired body mass following the programme (26.40 kg/m2). The observed changes confirmed the importance of physical activity for increasing health potential and preventing chronic diseases, including obesity and its complications, through, among others, improvement of energy balance and reduction of body mass, especially fat tissue, the mechanisms of which are indicated in the literature on the subject [3, 30, 31]. In turn, in other studies on the impact of a three-month aqua pilayoga exercise programme (twice a week for 60 minutes) on the somatic indicators of women above the age of 60, it was shown that after three months, there were positive changes in some somatic indices, including a decrease in BMI and a reduction in the amount of body fat with an increase in fat-free mass [32]. In further research on the relationship between physical activity and body composition it was also found that a higher level of physical activity was associated with lower body fat content, especially in women over 65 years of age [33]. Associations between an active lifestyle (taking part in physical activity at least 150 minutes per week) with a lower BMI has also been demonstrated among older women in sub-Saharan African countries [34]. Studies in the Spanish population also allowed to confirm the influence of the use of a Mediterranean diet with reduced energy value and physical activity on improving the body composition of people between the age of 55–75 [35].
With regard to the objective of the work, after 9 months of implementing the pro-health training programme, significant, positive changes were observed in four (out of six) indicators of women’s functional fitness level. A significant increase in the level of functional fitness was found, including the following tests: 30-second chair stand, 30-second arm curl, back scratch, and the 2-minute step-in-place. The described positive changes were, respectively, confirmed by an increase in the following: strength of the lower body (pelvic and lower limb muscles), upper body strength (upper limb muscles), mobility, flexibility of the upper body, as well as endurance and exercise tolerance. However, there were no significant changes in fitness tests regarding lower body flexibility, agility, or dynamic balance. The results of evaluation studies conducted as part of the first edition of the project correspond to the obtained regularities. In the cited studies, positive changes were also shown in functional fitness after 3 months of active participation in a health training programme, which included, in particular, increases in lower and upper body strength, lower and upper body flexibility, as well as exercise endurance and tolerance. In other Polish studies, it was shown that, as a result of health training in the form of aqua pilayoga (3 months, twice a week for 60 minutes), there was an increase in functional fitness indicators, including an increase in explosive strength of the upper and lower limbs as well as endurance and exercise tolerance in senior women [32]. In Brazilian studies, a positive effect of Pilates training lasting 16 weeks (twice a week, 60 minutes each) was also demonstrated on functional fitness indicators, including increased flexibility of the upper and lower body and the strength of the upper and lower limbs [36]. The importance of recreational physical activity, including cycling, running, walking, gym training, aerobics, and dancing, for maintaining and increasing functional fitness in older age, was also confirmed by research among seniors aged 65–75 years from Bremen, Germany [37]. The obtained results generally confirm the significance of physical activity with health training characteristics for improving various health indicators, including the functional fitness of older people, which was also indicated by the authors of other studies [33, 38]. This is particularly important in older people whose functional abilities decline, which makes it difficult to perform activities of daily living safely and effectively [20]. The achieved results correspond to the conclusions drawn on the basis of research by Spanish and Portuguese authors among older women, noting that physical activity of at least moderate intensity helps improve functional competences, including lower body strength, dynamic balance, and aerobic endurance, to maintain or increase muscle strength [39].
Due to the relationship between satisfaction with life and quality of life, changes in both of these variables will be discussed together. In this regard, it was found that after 9 months of active participation in the health training programme, a slight increase in the level of satisfaction with life did not reach the level of statistical significance. However, the quality of life profiles changed significantly positively, with an increase in 3 aspects concerning quality of life (somatic, psychological, and environmental), with the psychological aspect being the most intense, which was also the highest-rated dimension after completion of the programme (next to the environmental dimension). The social aspect did not change during the programme, probably due to the specificity of the group of surveyed women, because they were socially well-functioning individuals, involved in social life, and are most willing to participate in this type of programme. Furthermore, the social dimension of the quality of life concerns the assessment of social relationships, intimate life, and support from friends. However, it should be emphasised that the level of the psychological factor improved, i.e. well-being after the programme was higher among the respondents compared to the pre-start level. The obtained results indicate the importance of recreational physical activity for improving the quality of life in many aspects, especially in the psychological dimension. This confirms the impact of health training on optimising mental state, including by reducing stress as well as mental tension, and improving self-esteem. It also fits into the role of recreational physical activity as a factor improving health from a holistic perspective. In Korean studies, it was shown that older people who systematically engage in physical activity are less likely to suffer from depression than those who are physically inactive, which corresponds to the results discussed [40]. Meta-analytic studies have also confirmed the importance of yoga for improving the mental well-being of older people [41]. In other studies, it has also been demonstrated that high and moderate levels of physical activity have a very positive relationship with health-related quality of life in people with chronic diseases aged 65 years and above [42]. Associations between moderate physical activity and improved quality of life have also been reported in menopausal women aged 50–60 years [43]. Also, among older women (80+ years) from rural areas, the importance of physical activity, especially of moderate and high intensity, for physical health, general well-being, and greater satisfaction with life, has been demonstrated [44]. Associations between the Baltic Sea diet and physical activity with life satisfaction have been demonstrated in elderly women from Finland [45]. Moreover, in Portuguese and Brazilian studies, the positive impact of resistance training has been shown on quality of life profiles among older women [46]. Positive associations between increased physical activity and satisfaction with life among seniors have also been demonstrated by research carried out in Taiwan [38]. Also, research among women aged 45–64 years in Korea confirmed positive relationships between physical activity and various domains of quality of life, with the authors suggesting that physical activity in middle age is a significant element influencing the quality of life in old age [47]. American research has also confirmed the significant, positive importance of moderate and intense activity for the mental health and quality of life of seniors [7].
Generally, it may be summarised that the trends described in the discussed research partially positively verified the adopted research hypothesis. It was shown that active participation in the health training programme over a period of 9 months influenced, among others, a decrease in BMI, an increase in the level of functional fitness, and improvement in quality of life among women. The obtained results, corresponding to the results of other studies, confirm that physical activity can be treated as a factor improving the health of older women, which is also pointed out by other authors [11, 30, 31, 39, 43–47].
The research conclusions directly apply to women 60+ years of age from the population of Kraków participating in the organised health training programme. However, health is a universal value, and lifestyle, including recreational physical activity, is one of the key factors determining health potential, regardless of geography. Therefore, work on the significance of health training for various aspects of holistically understood health seems to be of a supra-regional dimension.
The strength of the study is assessment regarding the significance of participating in an organised health training programme by women aged 60+ years for health from a holistic perspective, taking both physical (BMI and functional fitness) and psychosocial dimensions (satisfaction and quality of life in 4 domains) into account. The limitations of the work primarily result from the self-report nature of some research tools, failure to take into account age as an additional variable, the small size of the group, as well as the characteristics of the group consisting of women voluntarily participating in the active health promotion programme, which does not allow the results to be transferred to a broader female population of senior age. The age variable was included only for BMI. Furthermore, the potential influence of other lifestyle factors on the analysed dependent variables cannot be fully excluded. It should be emphasised, nonetheless, that women declared no changes in their diet as a potential disturbing factor. Further work could concern the impact of the undertaken health training programme on a broader spectrum of somatic features (including body composition), balance, and personal resources. In future research the relationship between diet quality, nutritional status, bone density, functional capacity, psychological characteristics, and quality of life in older women engaging in recreational physical activity could also be examined.
Conclusions
Women aged 60+ years participating in the 9-month, organised, pro-health training programme showed a significant decrease in BMI and an increase in functional fitness in terms of muscle strength of the upper and lower limbs, flexibility of the upper body, as well as endurance and exercise tolerance. The decline in average BMI was beneficial regardless of age, as women below the age of 65 years reduced their degree of overweight, and women 65+ years old achieved the desired body mass.
Active participation of women 60+ years old in the 9-month, organised, pro-health training programme contributed to improving quality of life profile with regard to somatic, psychological, and environmental aspects, especially in the psychological sphere.
The obtained results generally confirmed the positive impact of systematic recreational physical activity with the characteristics of health training on various indicators of holistically defined health and quality of life among women above the age of 60 years.