Cancer is currently the second cause of death in many countries, including Poland [1, 2]. Importantly, some of the deaths caused by cancer could be avoided by effective prevention, early diagnosis, adequate treatment, and rehabilitation [3]. It has already been established that late diagnosis of neoplastic disease has a negative impact on the prognosis. Many causes of delay in diagnosis have also been identified. This may be due to the following: insufficient knowledge of the population, cultural differences, incorrect beliefs, superstitions, fear, or embarrassment [4–10]. It was shown that this group of diseases leads the highest level of anxiety among the respondents [11]. Moreover, according to the results of another survey conducted in Poland, 66% of Polish women indicated anxiety as the reason for not undergoing screening mammography [12].
Despite the fact that many activities have been undertaken to enhance both the first and second phase of prevention, cancer remains an unresolved (and even growing) problem of public health. Recently, the situation may have additionally been worsened by the COVID-19 pandemic [13].
The significant increase in the incidence (sometimes even called ‘epidemic’) of skin cancers (including melanoma and other non-melanoma skin cancers) together with population ageing and new survival-prolonging treatment modalities have influenced the establishment and further evolution of a new discipline, which is dermato-oncology. Despite the fact that it comprises a group of preventable diseases with known risk factors [9], a 45-fold increase of melanoma (and 80-fold of non-melanoma skin cancers) is expected over 8 decades. Australia is probably the only country that has managed to change this negative trend of melanoma incidence [14].
Skin cancer involvement may be a part of local invasion as well as distant metastatic evolution. Although the skin is a relatively rare location of cancer metastasis, it is becoming more and more common as a result of better treatment resulting in longer overall survival. The presence of skin metastases is most often found in late-stage cancer, but may also be the first symptom. It has been estimated that it may affect as many as 1 in 10 patients [15, 16]. Melanoma and lung cancer were reported to be the most common sources of skin metastases in men, and breast cancer in women. The clinical manifestation of neoplastic lesions within the skin is diverse (most often the form of nodules) and may be a challenge for doctors, including oncologists and dermatologists [15, 16].
There are still some neoplastic cases that are neglected, which are a clear examples of extreme delays in seeking medical advice and thus diminishing the chances of timely treatment. Many patients have symptoms, the recognition of which does not require any sophisticated research, being visible to patients and their relatives. As a consequence of negligence, it was impossible to apply radical treatment, which obviously made the prognosis unfavourable.
In the group of Polish breast cancer patients, anxiety was the most common reason for delaying a medical consultation (Figures 1 A, B). Another study, carried out in 6 cancer centres in Poland, concluded that the waiting time for treatment of cancer patients is too long and that it depends on the type of cancer and health care system [17]. What may seem surprising is that research from Spain has shown that diagnostic delay due to the health care system may not be related to the stage or prognosis of colorectal cancer [18]. According to a more recent study, in the current epidemiological situation, the interruption of colorectal cancer (CRC) prevention is expected due to COVID-19 disease, leading to the diagnosis of CRC in a more advanced stage [18].
Figure 1
A – Advanced left breast cancer (cT4N1M1). A 53-year-old female pharmacist living in the countryside (married, with 2 children) had been watching the growth of her left breast for several years. The patient was afraid of an oncological diagnosis, so she did not see a doctor or inform her family. Within the left breast, there is an infiltrative tumour accompanied by a board-like skin infiltrate, with a tendency to erythema, and an orange-peel symptom with numerous scaly lesions accompanied by yellow scabs in the course of advanced breast cancer with secondary skin involvement. The histopathological (HP) examination showed infiltrative breast cancer (oestrogen and progesterone positive, HER2 +++, Ki 67 20-30%). B – Advanced right breast cancer (cT4N1M1). A 49-year-old unemployed woman, with elementary education, living in the countryside with her husband and 2 children, had observed an increase of a right breast tumour for several months. The patient’s family (husband) was aware of the situation but was unable to convince her to see a doctor. The patient was afraid of being diagnosed with neoplastic disease. In the area of the right breast, a huge, necrotic tumour with a diameter of 20 cm was found, with a tendency to disintegrate and bleed, to form rocking granulation tissue, with numerous fissures and ulcerations filled with pus and fibrin. The infiltrative tumour compressed the armpit and infiltrated the surrounding tissues of the right armpit, décolletage, and the adjacent subcostal area diagnosed as advanced breast cancer with the secondary skin involvement. HP examination confirmed infiltrating breast cancer (oestrogen and progesterone receptor positive, HER-2 negative, Ki67 30–40%)

Numerous authors highlight the role of psychological factors causing the lack of engagement in pro-health behaviour in the event of unambiguous disease signals. Da Silva et al. demonstrated how women with breast cancer used excuses not to attend check-ups, avoided touching their breasts, and even avoided using the word “cancer” [19]. The authors also associated these behaviours with denial reaction which in effect caused the delay in early diagnosis.
In another study of 156 patients with oral squamous cell carcinoma Panzarella et al. showed that cognitive and emotional factors, especially denial of the disease, are the main reasons for patients failing to consult a physician, while there was no statistically significant association with lesion symptoms, sociodemographic characteristics (with the exception of age), and health-related variables [20].
The denial reaction to illness is a defence mechanism in which the patient does not acknowledge the disease despite the available information and their intellectual capacity to compile it [21]. The reaction is subconscious and is caused by the patients’ fear. A patient responding with a denial reaction has a partial, vague awareness of their symptoms. The patient employs a denial reaction to their illness because they sense fear, mental destabilization, and other hazards that will be triggered by the full realization of the disease.
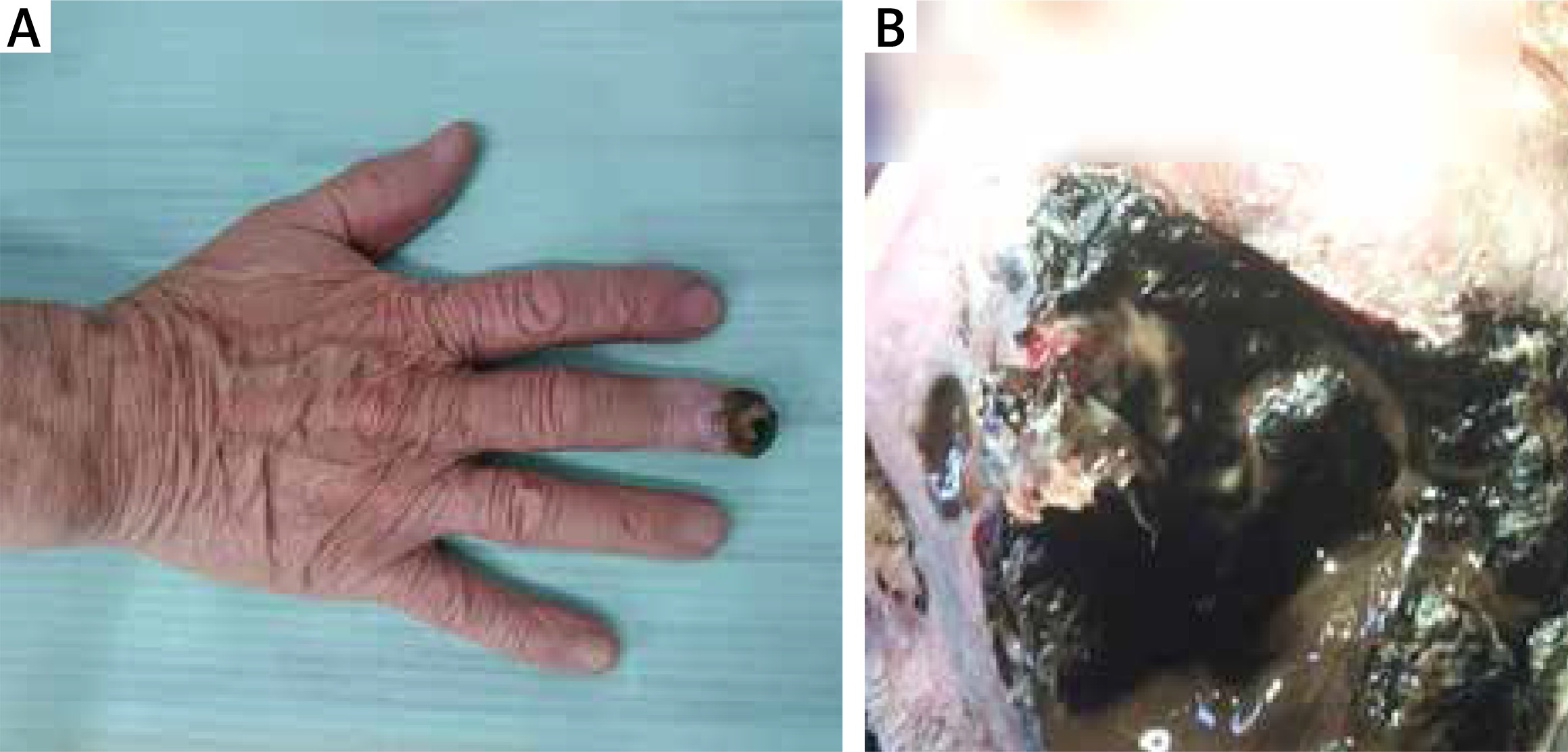
The diagnosis of cancer itself is often the primary cause of fear. It is still a common view that a cancer diagnosis is a ‘death sentence’ – in the study by Tejeda et al. as many as 25% of 181 women found the following belief to be true: “It doesn’t really matter if you get treated for breast cancer, because if you get it, breast cancer will kill you sooner or later” [22]. Patients are also afraid of anti-cancer treatment, which they associate with pain, disfigurement, and isolation from their loved ones [23] (Figures 2 A, B). Among some societies, fear of medical institutions and doctors is also dominant [24]. Moreover, the acknowledgment of the disease is associated with the loss of the current self-esteem and self-image as a healthy, strong, and independent person. Patients’ fears relate not only to themselves but they can also apply to families (e.g. fear of leaving children behind) [25]. The aforementioned fears underlie the denial reaction and are associated with a delay in undertaking pro-health behaviours when disease symptoms appear. However, some authors also emphasize the beneficial aspects of denial – in cases of terminally ill patients. Those patients, while not aware of the seriousness of their situation, experience less anxiety, allowing for better quality of life despite the impending end of life [26, 27].
Figure 2
A – Subungual melanoma pT4b. A 73-year-old single male patient, living in the countryside, with secondary level of education was admitted to the Oncology Clinic due to a bleeding, extensive ulcerative black tumour within the distal phalanx of the right third finger. In the interview, the tumour had been developing for several months, ignored by patient, who was afraid of surgical excision. Initially, he considered the tumour as post-traumatic haematoma. The patient repeatedly removed the tumour and the nail plate himself, which resulted in its growth. Clearly visible black hyperpigmentation is found within the dorsal and bulbar surfaces of the distal phalanx of the right hand, with a light pink infiltration, exfoliation, and complete destruction of the nail plate in the course of the subungual melanoma approved in the HP (pT4b). B – Stage III skin melanoma (inoperable). A 78-year-old male, widowed, city inhabitant, with secondary education, currently retired, came to the Oncology Clinic for the first time in 2014 because of an infiltrative, black solid tumour 3 cm in diameter, localized in the left cheek area, clinically suggesting a diagnosis of melanoma. The patient did not come for the biopsy, delaying the diagnostic proceedings for another 30 months. He did not want to undergo surgical procedures and potential oncological therapy. A large infiltrative-decaying tumour was seen within the left cheek, pressing on the lower eyelid, eye socket, penetrating into the maxillary sinus, filled with necrotic masses, thick mucus-bloody discharge. In the vicinity of the tumour, there is a purple swelling and black discoloration. In November 2016, a core-needle biopsy of a giant cheek tumour and a fine-needle biopsy of submandibular lymph nodes were performed. The histopathological examination confirmed the presence of melanoma metastasis in the left submandibular node. Because the patient did not agree to further diagnostics, it was not possible to assess the staging of the disease according to TNM. He also did not agree to be hospitalized or to receive systemic treatment
According to the results of the latest population-based study, “EUROCARE-5”, the results of cancer treatment in Poland are inferior to the European average. Stage at diagnosis, cancer biology, access to healthcare, efficiency of screening, and diagnostic workup are listed among possible reasons for the registered differences between European countries. Other possible factors highlighted include the following: socioeconomic, lifestyle, and general health [28]. More recent data from the EUROCARE-6 study are yet to be published. Another analysis of EUROCARE-5 identified other disparities. The authors concluded that patients from Eastern Europe were diagnosed at later stages and had worse 5-year relative survival and greater relative excess risk of cancer death compared to patients from other parts of Europe. Inferior equipment, less comprehensive diagnostics, and less access to anti-cancer therapies could lead to less efficient care [29]. In addition, low level of knowledge, anxiety, embarrassment, as well as misconceptions and financial aspects have been listed as the main barriers to cancer prevention, early diagnosis, and implementation of cancer treatment [11, 30, 31].
Importantly, breast cancer and melanoma belong to the increasing in number group of cancers in which early detection impacts prognosis significantly [32, 33]. Patients diagnosed with melanoma at stage 0-I have a 5-year survival of 92–100%, while only 15–20% of those diagnosed at stage IV would survive for a 5-year period [33]. Late diagnosis is also associated with significantly higher treatment costs. For example, in Australia the average cost of annual treatment of a single patient was 1175 USD for 0/I/II stage of melanoma, while it was as much as 80, 440 USD for unresectable III/IV stage [34]. Factors associated with late-stage diagnosis of melanoma include the following, among others: gender (male), level of education (lower), race, and ethnicity (other than non-Hispanic) [33]. According to a more recent study, in the current epidemiological situation, the interruption of CRC prevention is expected due to COVID-19 disease, leading to the diagnosis of CRC at a more advanced stage [35].
It has already been demonstrated that improving general public knowledge could enhance cancer prevention, among others by reducing the level of anxiety [11]. Given the above, further actions in the field of public health are necessary to increase public awareness of all areas of prevention.
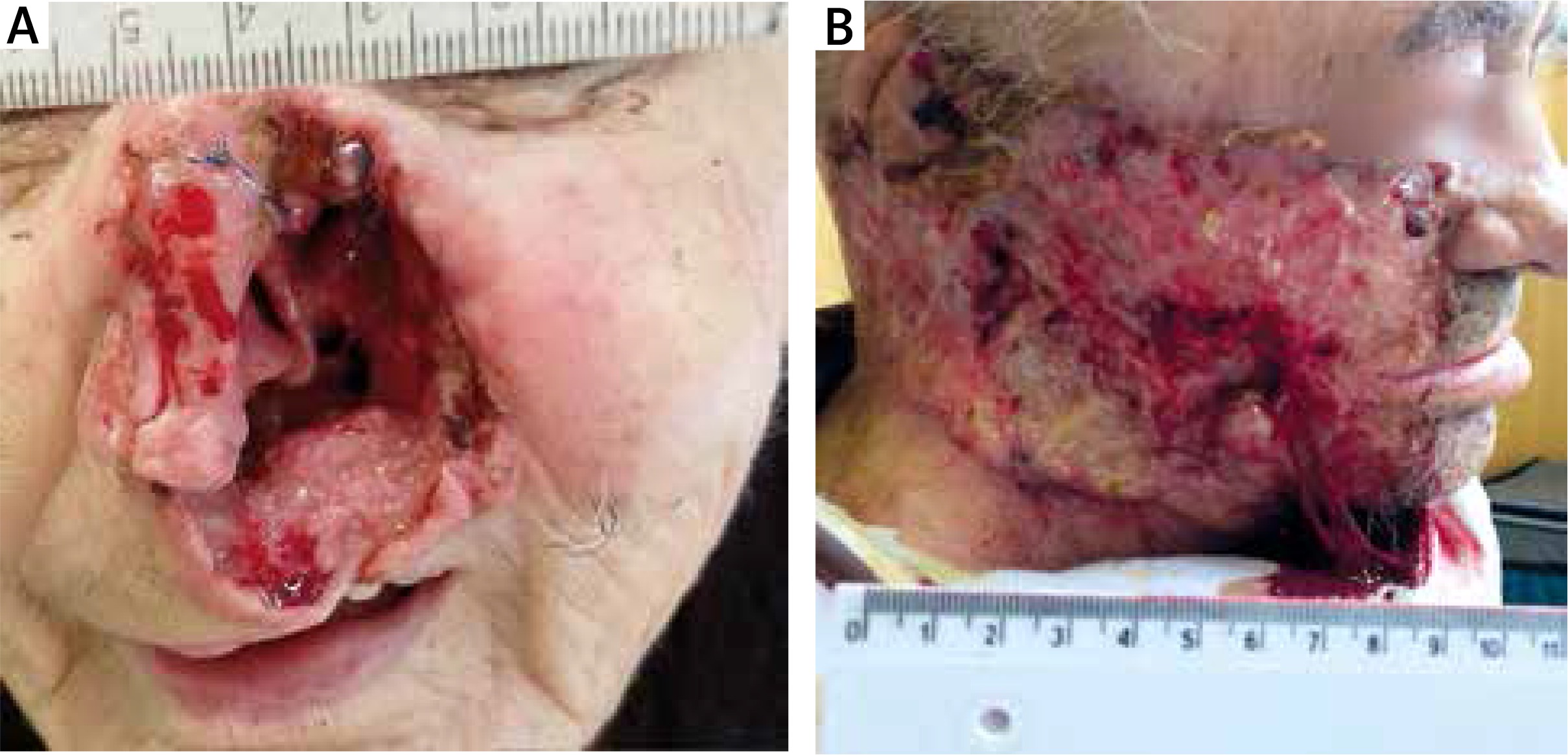
The key aspect for the patient to undertake oncological treatment is to inform about and discuss the advancement of the disease, therapeutic possibilities, and prognosis. This allows informed consent to be obtained from the patient regarding the proposed treatment. Unfortunately, many oncological patients remain superstitious: “Better do not touch” [36], which inhibits the patient from taking further, rapid therapeutic steps (Figures 3 A, B). The role of the physician is to change this attitude in cancer patients.
Figure 3
A – Basal cell carcinoma-locally advanced. A 78-year-old retired woman with primary education, living in the city with her husband, had observed the growth of tumour of the nose for 15 years. Despite her daughter’s repeated requests, she did not go to the doctor. She was afraid of the surgical procedures. Extensive infiltration, ulceration with destruction of the left nasal wing, nasal bridge, and turbinates, with penetration into the left maxillary sinus in the course of locally advanced basal cell carcinoma confirmed BCC. Due to the lack of the possibility of applying local treatment, the patient was qualified for treatment with vismodegib and is currently undergoing this treatment. B – Basal cell carcinoma-locally advanced. A 68-year-old retired man with basic education, living in the countryside, married, had been observing a tumour of the right side of his face for several years. Despite repeated requests from his family, he did not go to the doctor (he was afraid of the final surgical procedures). Extensive ulceration covering the right part of the face with destruction of the lower eyelid of the right eye, right auricle, with destruction of the muscular fascia, with infiltration of the occipital area and the nape in the course of locally advanced basal cell carcinoma were proven also in histopathological assessment. Due to its advanced stage and the inability to perform local treatment, a systemic therapy with vismodegib was initiated