





SARS-CoV-2-associated pneumonia requires intensive care treatment in up to 21% of affected patients [1, 2]. For this subgroup of patients, treatment of coronavirus-19 disease (COVID-19) routinely encompasses oxygen supplementation and non-invasive ventilation followed by invasive ventilation in the case of further clinical deterioration [3, 4]. High-flow nasal cannula (HFNC) is a relatively new form of oxygen application, routinely used in patients with hypoxaemic respiratory failure [5–7]. It allows a constant fraction of oxygen to enter the airways and facilitates an improved oxygenation by washing out the carbon dioxide and reducing the dead-space ventilation. This easy-to-apply and tolerable respiratory support is often considered a helpful tool to avoid standard non-invasive ventilation forms, characterized by a lower tolerability and higher risk of complications [8].
In the context of the current pandemic, preliminary reports highlighted the role of HFNC in the treatment of COVID-19-induced respiratory failure. The treatment effectiveness of patients recovering without the need for invasive ventilation ranged between 50.0% and 87.5% [9–11]. Risk factors for a HFNC treatment effectiveness are still insufficiently characterized.
Based on these considerations, the aim of this study was to highlight the clinical, laboratory, and cardiorespiratory parameters that might predict the effectiveness of HFNC treatment in patients with severe COVID-19.
METHODS
This retrospective single-centre study was approved by the Local Ethics Committee of the Ludwig-Maximilians-University, Munich (#20-618 and #20-853). Due to the retrospective nature of the study and irreversible anonymization of the collected data, the requirement for written informed consent was waived by the Ethics Committee. The present study was conducted at the Asklepios Lung Clinic, Munich-Gauting, Germany, after local hospital approval.
Sixteen patients admitted between 16 March and 3 June 2020 tested positive for SARS-CoV-2 and required HFNC therapy. Clinical data were collected from available internal medical records. The effectiveness of HFNC was assessed by clinical, laboratory, and cardiorespiratory monitoring. Accordingly, the patients were divided into 2 groups: in Group 1, patients recovered successfully upon HFNC (efficient HFNC), whereas patients in Group 2 experienced a further respiratory deterioration upon HFNC. Group 2 included patients who a) required an invasive ventilation upon HFNC failure and b) did not agree with an escalation of the intensive care measures after informed medical consent and thereafter experienced a COVID-19-related, multi-organ dysfunction and died.
The admission criteria to the Intensive Care Unit (ICU) were based on the guidelines of the Society of Critical Care Medicine and respected the availability of intensive care resources during the COVID-19 pandemic [12, 13]. Eligibility criteria for HFNC were as follows: an oxygen saturation (SpO2 ) < 90%, hypo-xaemia (corrected partial pressure of oxygen/PaO2 < 55 mmHg) with 4 L oxygen supplementation (fraction of inspired oxygen/FiO2 = 0.36), respiratory rate > 25 min–1, and hyperventilation (pCO2 < 35 mmHg). Uncompliant patients experiencing a haemodynamic instability or pulmonary oedema were not considered eligible for HFNC therapy.
High-flow nasal cannula therapy was performed with a HAMILTON-C6 mechanical ventilator (Ha-milton Medical AG, Bonaduz, Switzerland, www.hamilton-medical.com) with the following initial settings: oxygen supplementation flow of 40 to 50 L min–1 and FiO2 0.4 to 0.5.
In order to evaluate the disease severity, low-dose volumetric, thin-slice CT scans were performed upon admission to the hospital. Based on the CT imaging, the parenchymal damage of the affected lobes was assessed by an experienced board-certified radiologist. The calculated CT severity score (0–25 points) according to the extent of lobar involvement respected the previously described protocol [14]. Patients with delayed CT examinations or without informed medical consent for a CT scan were not included in the analysis.
Results on day 0 and 4 after initiation of HFNC are presented as median values with interquartile range (IQR, 1st–3rd quartile). Comparisons between groups were performed by using the Mann-Whitney U-test for continuous data, and c2 test for categorial variables, taking a significance level of P < 0.05 into account. Receiver operating characteristics (ROC) and Youden’s J statistic were used to determine cut-off values for the analysed parameters. Statistical analysis was performed by using SPPS (Version 25, IBM, Armonk, New York, USA).
RESULTS
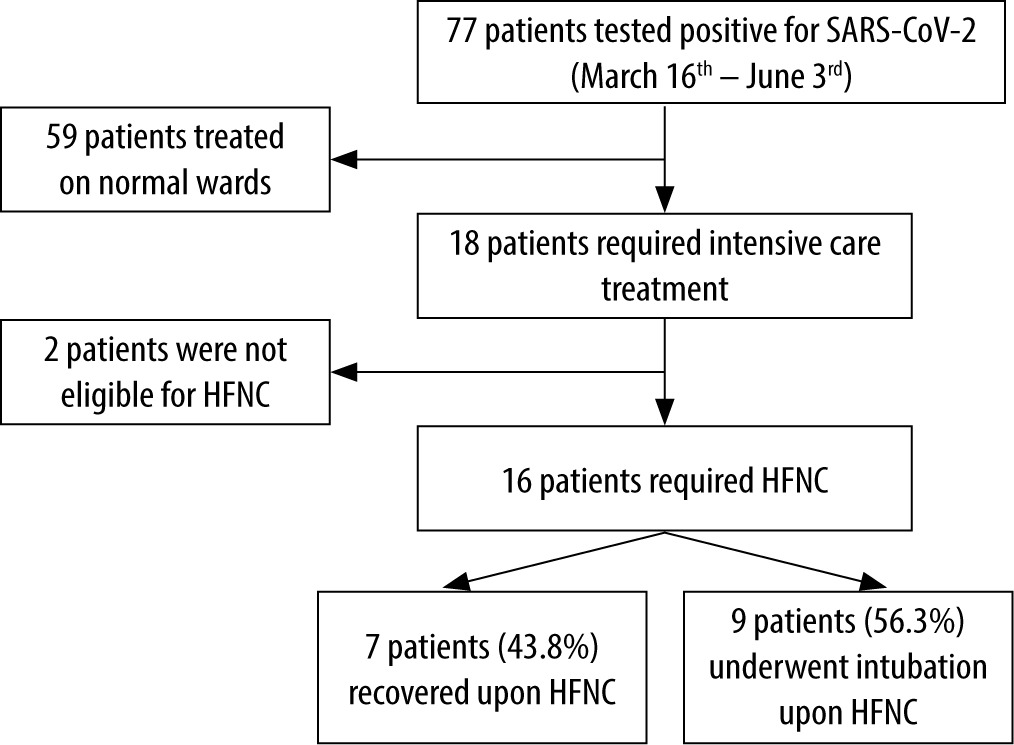
Seventy-seven patients with positive test results for SARS-CoV-2 were admitted to the Asklepios Lung Clinic Munich-Gauting, Germany between 16 March and 3 June 2020. Eighteen patients (23.4%) experienced a severe course of disease, whereby 16 patients (median age 78.5 [61.25–81.0] years, 31.3% female, median body mass index (BMI) 24.69 [23.73–31.97] kg m–2) required HFNC therapy (Figure 1). Seven patients (43.8%) recovered successfully upon HFNC (Group 1), whereas 9 patients (56.3%) required invasive ventilation (Group 2). In Group 2, 5 out of 9 (55.6%) patients died upon disease progression and HFNC failure.
FIGURE 1
Flow chart showing the severity of COVID-19 patients admitted to the Asklepios Lung Clinic Munich-Gauting, Germany during the first wave of the pandemic, and their responsiveness to high-flow nasal cannula therapy (HFNC)
Both groups did not differ in terms of age, sex, BMI, and comorbidities (Table 1). No significant differences of symptoms were reported in both groups, with the most prevalent symptoms being fever (71% vs. 67%), dyspnoea (43% vs. 78%), and dry cough (86% vs. 78%) (Table 2).
TABLE 1
Demographic data of COVID-19 patients upon admission to the ICU or general ward, categorized by high-flow nasal cannula (HFNC) treatment effectiveness. Median values with interquartile ranges are reported. For age, BMI, and total length of stay the Mann-Whitney U-test was used. For sex and mortality, a c2 test was used, with a significance level of P < 0.05*
TABLE 2
Comparative analysis of clinical symptoms upon admission in patients undergoing high-flow nasal cannula (HFNC) treatment. Comparisons were performed by using the χ2 test, with a significance level of P < 0.05*
General assessment scores for disease severity included the Sequential Organ Failure Assessment score (SOFA), the Acute Physiology and Chronic Health Evaluation score (APACHE II) as well as Intubation Risk score (ROX). No significant differences in the SOFA score, APACHE II score, and ROX score were observed in both groups (data not shown). In addition, the CT severity score was not significantly associated with a failure of the HFNC treatment (median 7 [6–14] vs. 16 [5.5–20], P = 0.299). The CT severity score divided patients with severe and non-severe course of disease into 2 groups. However, no association between parenchymal damage and HFNC failure was reported. Patients requiring invasive ventilation presented a significantly elevated body temperature on day 4 (38.5 [38.0–39.4]°C) when compared to patients who successfully recovered upon HFNC (36.5 [31.1–37.1]°C, P = 0.010). A lower MAP on day 4 was significantly linked to HFNC failure (77.7 [55.7–79.8] mmHg vs. 91.8 [85.3–99.5] mmHg, P = 0.030). Oxygen saturation on day 4 was significantly reduced in Group 2 (88 [79.5–90.0]%) in comparison to Group 1 (95 [90–96.3]%, P = 0.017). Retrospectively, patients experiencing a HFNC failure had a significantly increased oxygen demand already on admission with a higher median FiO2 of 0.72 [0.54–0.76] vs. 0.46 [0.31–0.54], P = 0.022) and a lower median PaO2/FiO2 of 93.3 [67.2–145] vs. 115 [111–201], P = 0.042). Laboratory analysis on day 4 revealed significantly increased CRP levels in patients requiring invasive ventilation in comparison to the patients who successfully recovered upon HFNC (270 [205–463] mg L–1 vs. 50.1 [18.9–70.4] mg L–1, P = 0.029; Table 3). ROC analyses identified a serum CRP level > 108 mg L–1 on day 0 (area under curve (AUC) 0.929, P = 0.005) and FiO2 of > 0.58 (AUC 0.881, P = 0.022) to predict disease severity and consecutively HFNC failure on day 4.
TABLE 3
Laboratory tests of COVID-19 patients upon admission and on day 4 after initiation of high-flow nasal cannula (HFNC), categorized by HFNC treatment effectiveness. Laboratory parameters of COVID-19 patients undergoing a successful HFNC were compared to those of patients requiring invasive ventilation upon non-effective HFNC therapy. Median values with interquartile ranges are reported. All comparisons were performed by using the Mann-Whitney U-test with a significance level of P < 0.05*
In addition, persistent oxygen saturation < 89% and PaO2/FiO2 ratio < 91 on day 4 were identified as significant predictors for HFNC failure (AUC 0.933, P = 0.018 and 0.893, P = 0.038, respectively).
Patients with successful HFNC required a shorter period of hospitalization on ICU (0 [0–5] days) in comparison to patients experiencing a HFNC failure with consecutive orotracheal intubation (5 [0–38.5] days). In Group 2, 5 patients died. No fatalities were reported in Group 1 (Table 1).
DISCUSSION
HFNC therapy is an efficient non-invasive oxygen supplementation method for the treatment of pneumonia-induced type 1 (hypoxaemic) respiratory failure [15–17]. Preliminary reports underlined the role of HFNC as alternative respiratory support in the treatment of COVID-19-related respiratory failure. However, factors predicting HFNC effectiveness in patients with COVID-19 pneumonia are still insufficiently characterized. For this reason, our observational study analysed the efficiency of HFNC therapy as an alternative for invasive ventilation. Sixteen severe COVID-19 patients undergoing HFNC at the Asklepios Lung Clinic Munich-Gauting, Germany during the first pandemic wave were retrospectively analysed. No significant differences in terms of sex, BMI, and metabolic and cardiorespiratory comorbidities were reported between Group 1 and Group 2. Although preliminary studies identified older age, male sex, increased BMI, and diabetes mellitus as risk factors for a severe course of disease, biometrical characteristics and comorbidities do not seem to be indicative for HFNC effectiveness [18–22]. Only Xia et al. [21] found male sex to be associated with HFNC failure. In our study, 10 of 16 patients requiring HFNC were 70 years old or above. Advanced age constituted an inclusion criterium for HFNC, given the high rate of the reported ventilator-associated complications [19, 23].
In addition, an increased oxygen demand, as well as persistent fever or hypotension on day 4 characterized the patients requiring invasive ventilation upon HFNC failure. These findings are in line with Vianello et al. [20], who found the PaO2/FiO2 ratio to be a significant predictor of HFNC failure in 9 of 28 COVID-19 patients with severe hypoxaemia. A second report based on 43 patients found oxygen saturation to be an independent risk factor for HFNC failure leading to emergent intubation after only 3.5 hours of observation [22]. In addition, Kang et al. [24] similarly highlighted the association between hypotension and HFNC failure. We observed a prolonged ICU stay in patients experiencing a HFNC failure, in accordance with previous results reported by Xia et al. [21]; (25 days total length of stay). While efficient HFNC therapy was linked to a successful recovery of all patients, HFNC failure was associated with a case-fatality rate of 55.6%, in accordance with 60% reported by Vianello et al. [20] and 43.8% by and Li et al. [25]. Epidemiological and demographic heterogeneity might explain the wide range of mortality rates, i.e. 92% reported by Calligaro et al. [26] and 22% by Andino et al. [15]. Of note, the HFNC failure and fatality rate in our cohort could not be explained by differences in therapeutic regimen. All patients received low-molecular-weight heparins upon clinical admission. The use of corticosteroids in patients with severe COVID-19 was not routinely implemented during the first wave of the pandemic in our hospital. Only one patient with a history of combined pulmonary fibrosis and emphysema underwent a high-dose intravenous corticosteroid therapy and recovered after 21 days of HFNC therapy. No patient was treated with antiviral drugs (e.g. Remdesivir) because they were not widely available or recommended during the respective period.
Taken together, our study analyses the factors predicting the HFNC effectiveness in the treatment of COVID-19 patients. Specifically, fever (> 38.5°C), low blood pressure (MAP < 77.7 mmHg), a high fraction of inspired oxygen (FiO2 > 0.72), as well as high levels of serum CRP (> 108 mg L–1) on day 4 after initiation of the HFNC might predict negative outcomes upon HFNC therapy. Despite these promising results, our study is constrained by a small-numbered patient cohort, being a limitation of the study. On the other hand, our study started in March 2020, at the beginning of the COVID-19 pandemic in Bavaria, Germany. At that timepoint, no preliminary data or official recommendations on the effectiveness of HFNC in the treatment of COVID-19-induced respiratory failure were available. In addition, given the potential complications of the non-invasive ventilation, its tolerability, and risk of aerosol dispersion, the intensive care unit of our hospital decided to implement HFNC as novel respiratory support for COVID-19 patients admitted with respiratory failure. Consecutively, HFNC was implemented in all eligible patients admitted to the ICU upon respiratory deterioration.
Given the limited expertise and number of published reports on this topic, we believe that our study provides valuable preliminary findings on the effectiveness of HFNC and should therefore be further evaluated in larger prospective studies.
In addition, clinically relevant intensive care scores including SOFA, APPACHE II, ROX, and the CT severity score did not reveal significant differences between both groups in our study. The CT severity score divided patients with severe and non-severe course of disease into 2 groups. However, no association between parenchymal damage and HFNC effectiveness was reported.
An impediment to the standard application of HFNC in the clinical routine at the beginning of the pandemic was the risk of cross-infection due to environmental aerosol spreading [8, 27]. Because non-invasive ventilation was not routinely used during the first pandemic wave in the treatment of COVID-19-related respiratory failure, no previous experience was available at that time. Moreover, standard non-invasive ventilation techniques (NIV) and HFNC were considered comparable in the aerosol spreading potential [8]. For this reason, official recommendations advocated for invasive ventilation in the case of further deterioration upon HFNC [12].
In order to overcome aerosol dispersion and viral cross-contamination during HFNC therapy, all patients were hospitalized on the ICU in single-bed rooms or in destinated slots (9 m2 each) with at least 2 m distance between beds. In addition, intensive precautionary methods, including routine quantitative polymerase chain reaction (qPCR) screening and upon clinical suspicion, led to an efficient primary prevention with no further reported COVID-19 cases among patients or healthcare workers in the analysed period.
CONCLUSIONS
Taken together, HFNC can be considered as a safe non-invasive oxygen supplementation me-thod that might be an effective alternative for invasive ventilation in patients with a severe course of COVID-19 pneumonia. Parameters including decreased oxygen saturation, decreased PaO2/FiO2, as well as elevated serum CRP levels on day 4 after initiation of the HFNC might predict further clinical deterioration of patients followed by HFNC failure and consecutive intubation. Further multicentre prospective studies are necessary to validate these preliminary findings and the effectiveness of HFNC in the treatment of COVID-19-induced hypoxaemic respiratory failure.