





Dear Editor,
In late December 2019, SARS-CoV-2 was discovered, which is responsible for a new human disease called COVID-19. Among all laboratory-confirmed COVID-19 cases, 14% were hospitalized, with 2% admitted to intensive care units (ICU) with acute respiratory distress syndrome (ARDS) requiring mechanical ventilation [1]. SARS-CoV-2 has spread quickly across the world, with more than one hundred million confirmed cases and more than 2,500,000 dead. In March 2020, the Hospital of Valenciennes had to admit hundreds of COVID-19 patients, and its capacity was almost exceeded [2]. More recently, in France, thousands of critically ill patients had to be admitted to ICUs. In Europe, the next wave of COVID-19 pandemic could be more severe than the first one, and we already know that, in the case of increasing numbers of critically ill, some of them will die as a result of the unavailability of mechanical ventilators [3]. This shortage may be lessened if one ventilator could service more than one patient. The main worry is that this concept could be not useful and systematically deleterious for the patient. Some concepts have already been proposed to ventilate differently two circuits with a single ventilator, with several limitations like the lack of individualization of ventilation of each circuit [4–6]. More recently, in the face of the COVID-19 pandemic, Clarke et al. [7] described a new concept able to deliver specific ventilation for two different lung tests with a single ventilator. Again, Levin et al. [8] have recently shown that a similar concept of differential ventilation using a single ventilator with flow control valves is feasible in humans.
We would like to describe a different, novel, and cost-effective way of ventilating two patients with a single ICU ventilator using two circuits with different pressure controlled ventilation (Figure 1).
FIGURE 1
Pressure monitoring of our concept showing two different specific pressures in circuits with a single ventilator. We can observe on the single ICU-ventilator screen (A) that the inspiratory pressure is set at 35 mbar (A1) and the expiratory pressure is set at 5 mbar (A2). On the screen of the left monitor, we can observe the pressure in circuit B (B) with an upper pressure (B1 = 21 mbar) regulated with specific pressure regulator of circuit B, and a lower pressure equal to the expiratory pressure set on the ventilator (B2 = 5 mbar). On the screen of the right monitor, we can observe the pressure in circuit B’ (B’) with a different upper pressure (B’1 = 28 mbar) regulated with another pressure regulator on circuit B’, with the same lower pressure (B’2 = 5 mbar)

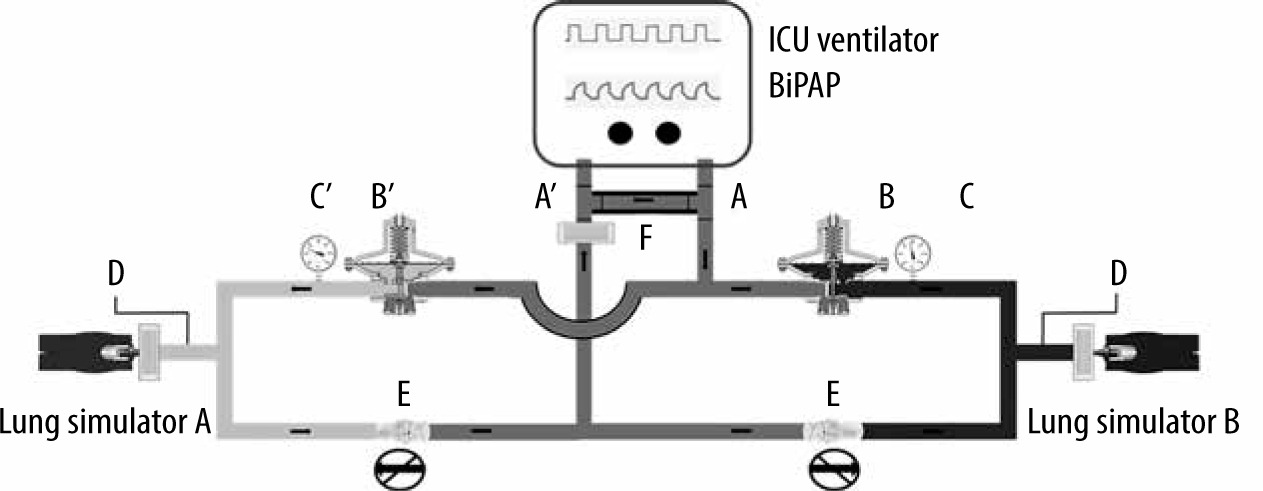
We connected to the inspiratory valve of an ICU ventilator a T-piece (Figure 2 – A). This piece was connected to a Y-piece of flextube and connected to two pressure regulators (pressure range of 16 to 34 mbar) (Figure 2 – B), followed by an analogue pressure gauge (Figure 2 – C) and a second flextube connected to the test lung. On the expiratory circuit, a one-way valve was used (Figure 2 – D), followed by another T-piece (Figure 2 – A’), and finally the exhalation valve. The two circuits were similar. There is also a necessary specific shunt between the two T-pieces of the inspiratory and the expiratory valves to allow high inspiratory pressures (Figure 2 – E).
FIGURE 2
Schema of our new concept based on ventilating two patients (lung A on the left and lung B on the right) with two distinct inspiratory pressure controls (light grey on the left and dark grey on the right) connected to a single ventilator. Important components are represented on the figure: the 3D-printed T-piece (A and A’), the pressure regulator (B and B’), the pressure gauge (C and C’), the non-return valve (D and D’), and the specific shunt (E)
We tested it using SelfTestLungs (STL) (Dräger, Lübeck, Germany) and a modified STL (mSTL) with an elastic band to decrease its compliance. A gas wall-powered Evita respirator (Dräger, Lübeck, Germany) with a Bilevel Positive Airway Pressure (BiPAP) mode was used. The upper pressure levels of each circuit were set with the pressure regulator, and the lower pressure levels were the same for both circuits. The pressures of both circuits were measured in each filter with an invasive blood pressure transducer and displayed on a specific monitor.
With two identical STLs and with a single upper pressure set on the ventilator, we showed that we can obtain two specific inspiratory pressures on each circuit regulated by pressure regulators (Figure 1). Moreover, the pressure of each circuit is independent.
With one STL and an mSTL, we observed that the delivered volume of each test-lung depends on the specific inspiratory pressure (set on a pressure regulator, and the upper pressure set on the ventilator is the same) and PEEP, with a high correlation between the two simulated lungs (r > 0.9, P < 0.05) and a very low standard deviation cycle after cycle. Finally, if we use one STL paired with mSTL as well as two identical STL, the global volume measured by the ventilator is equal to the sum of volumes of both test-lungs measured separately.
The concept has some limitations, such as the fact that the respiratory rate, the fraction of inspired oxygen, and the PEEP level are the same for both patients, also that both patients need to receive neuromuscular blockade to limit triggering or the lack of individual alarms. At the same time, this solution has several advantages: the possibility to individualize the level of inspiratory pressure in order to deliver a specific volume to each patient, the non-return valve which enables patients to be disconnected independently while also minimizing the risk of any cross-infection, and the possibility to practice prone position or cardiac arrest resuscitation on only one patient. Additionally, this solution is relatively inexpensive (less than €600 per device), easy to reproduce, and potentially adaptable to different models of ICU ventilators. The ventilator splitting strategy will never be as performant as using a single ICU ventilator for a single patient, especially for weaning. It should be reserved as a short-term emergency solution and be used as a “short bridge” to more conventional ventilation strategies.
Although we have not tested our device in experimental or animal studies yet, due to the urgency of the situation some administrations may allow this concept, to avoid some ethical choices [9]. Our concept based on ventilating two test lungs using two distinct inspiratory pressure-controlled circuits connected to a single ventilator seems to be viable and cost-effective and may be life-saving. This potential to increase the capacity of ICUs, which differs from the standard of care, should lead to an ethical debate: Should we (potentially less effectively) ventilate more patients or focus on selected critically ill patients with better prognosis?