
Introduction
Colorectal cancer (CRC) is the third most common type of cancer in the world, after breast and lung cancer in women and prostate and lung cancer in men. Colorectal cancer is also the fourth leading cause of death as a result of cancer. Unfortunately, the incidence of cancer of this organ is constantly increasing [1].
Bleeding from the gastrointestinal tract, abdominal pain or a change in bowel movements may indicate colon cancer. However, there is no precisely characterized pain in this condition and therefore the disease may develop unnoticed [2]. A person who notices the above-mentioned symptoms should see a doctor as soon as possible for diagnostic tests. To make a diagnosis, your doctor may order an imaging test, such as a colonoscopy. Digital rectal examination, CEA marker concentration in the blood or stool occult blood test are among the other diagnostic methods for colorectal cancer. It should be emphasized that early detection of this cancer provides a chance for complete cure [3]. However, despite screening tests and preventive measures, colorectal cancer is still a major challenge for modern medicine. The appearance of this cancer is a great stress, not only for the patient, but also for his family [4]. The quality of life of a sick person decreases significantly after diagnosis and depends on the impact of the disease and the treatment applied on the functioning of the patient and his loved ones in the physical, social and mental dimensions [5].
One of the typical features of the discourse on cancer prevention in Poland, there is a prevailing belief about the low level of knowledge of Polish women and men on the possibilities of reducing cancer incidence [6]. It is suspected that the belief that cancer awareness is low is the result of the experience of working doctors with patients. This is also evidenced by research on certain phenomena, including: dietary habits [7].
Aim
The aim of the study was to assess the level of knowledge of people coming to the Endoscopic Laboratory for colonoscopy examination about the risk factors of colorectal cancer.
Material and methods
The research group consisted of people residing in the Lodz Voivodeship who came to the Endoscopic Laboratory to undergo a colonoscopy examination. The study involved 238 randomly selected patients (136 women and 102 men). Participation in the study was voluntary and anonymous, about which respondents were informed on the first page of the survey. The diagnostic survey method was used, and the research tool was an own questionnaire. The research began in December 2023 and ended on February 20, 2024. The questionnaire included 18 questions examining the respondents’ level of knowledge about colorectal cancer risk factors and 4 questions regarding demographic variables. Before the study, the respondents were informed about the purpose of the study and gave informed consent to participate in it. The study was conducted in accordance with the principles of the Declaration of Helsinki.
In order to answer the research questions and verify the hypotheses, statistical analyzes were carried out using the IBM SPSS Statistics package version 29. With its help, basic descriptive statistics were calculated along with the normality of distribution test, numerous frequency analyzes and comparative analyzes were performed using the non-parametric Mann Whitney U test and Kruskal-Wallis. In this study, a p value < 0.05 determines the level of statistical significance.
Results
Table 1 presents the sociodemographic data of the participating respondents in a research.
Table 1
Sociodemographic data of the study group (N = 238)
Before starting the actual analyses, aimed at finding answers to the research question, two quantitative variables were developed. The first one concerned the level of knowledge about the possibility of colorectal cancer. This variable was created by summing the correct answers given to survey questions relating to specific issues related to the risk of colorectal cancer (eight questions in total). In the case of single-choice questions, respondents received one point for each correct answer.
In the case of multiple-choice questions, respondents had the opportunity to obtain a higher number of points, corresponding to the number of all correct answers within a given question (one point was awarded for each correct answer, and one point was subtracted for each incorrect answer - however, the number of points for a given question could not be lower than 0). Finally, the points obtained in each question were summed to create a knowledge level index. The second variable developed concerned the level of knowledge about risk factors influencing the development of colorectal cancer. The respondents received one point for correct answers to the question regarding this issue, and a negative point for an incorrect answer.
Then, basic descriptive statistics were calculated for the variables developed in this way, along with the Shapiro-Wilk normality test. These analyzes were carried out divided into groups based on gender, education level and age, which was dictated by the nature of the research questions. The obtained results are presented in table 2.
Table 2
Descriptive statistics with the test of normality of distribution for the tested quantitative variables divided into separate groups (N = 238)
The obtained results showed that the distribution of results for the variable relating to the level of knowledge about the possibility of developing colorectal cancer in most groups deviated significantly from the normal distribution, while for the variable relating to the level of knowledge about risk factors influencing the development of CRC in two groups it was inconsistent with a Gaussian curve. Therefore, taking into account the failure to meet the assumption of parametric tests of equal size of the compared groups, non-parametric tests were used for the comparative analyzes described in this chapter.
After analyzing the distribution of quantitative variables, we began to check the level of knowledge about CRC among the inhabitants of the Lodz Voivodeship who came to the Endoscopy Laboratory. For this purpose, basic descriptive statistics were calculated for the entire study group. The results of the analyzes are presented in table 3 and in a histogram (Fig. 1).
Table 3
Basic descriptive statistics regarding the level of respondents’ knowledge about the possibility of colorectal cancer (N = 238)
| M | Me | SD | Min. | Maks. | lower quartile | upper quartile | |
|---|---|---|---|---|---|---|---|
| Level of knowledge about the possibility of colorectal cancer | 8,79 | 9,00 | 2,09 | 5,00 | 16,00 | 7,00 | 10,00 |
Figure 1
Histogram including the results regarding the level of respondents’ knowledge about the possibility of colorectal cancer
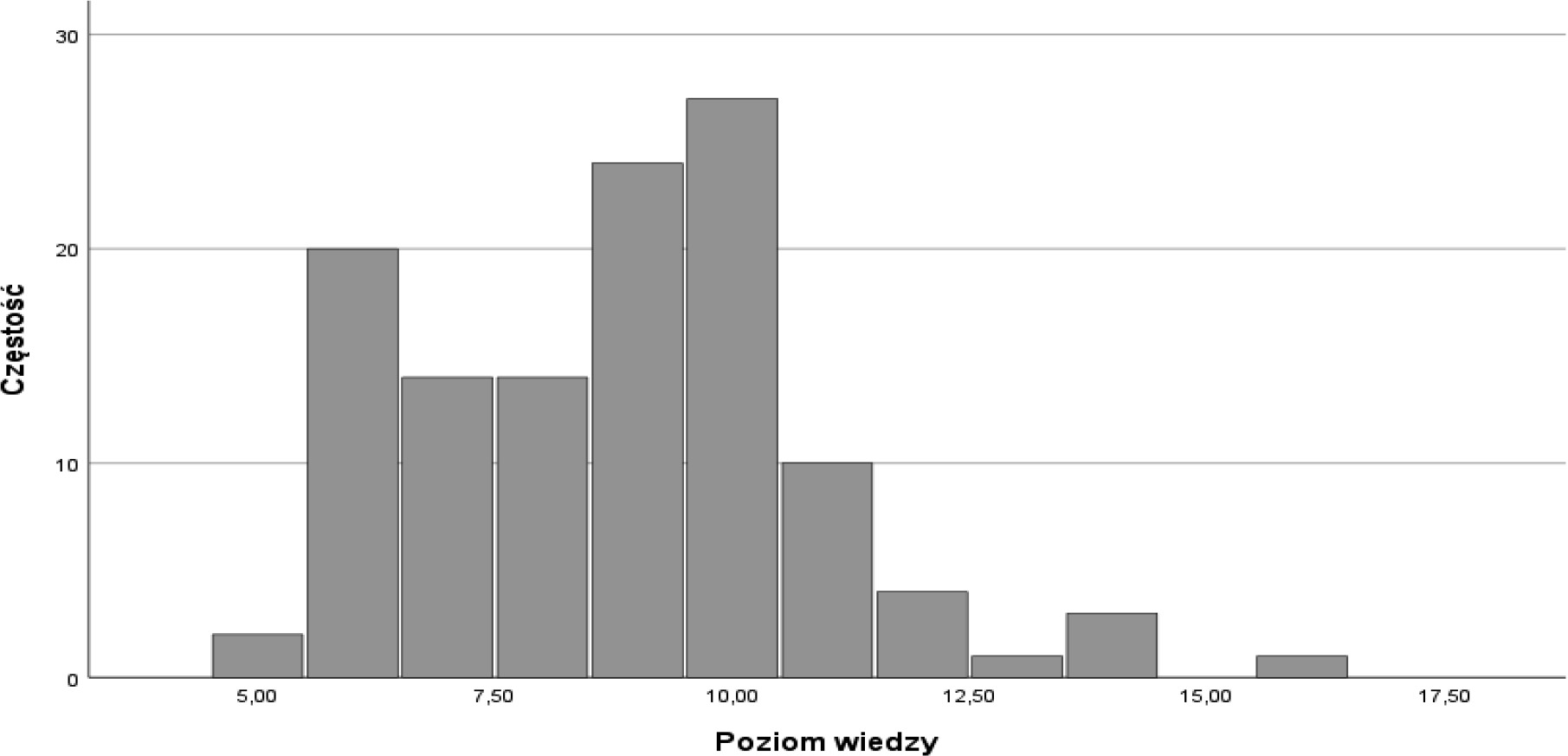
The statistical analysis of the study showed that the level of knowledge of patients undergoing colonoscopy regarding the possibility of CRC was rather low. The respondents obtained an average of 9 points in the knowledge test (out of 23 possible points). The weakest result in this group was 5 points, while the highest was 16 points. The median was 9.
Then, the influence of the respondents’ gender on the level of knowledge regarding CRC was analyzed. The data obtained showed that men had a significantly higher level of knowledge about CRC compared to women. However, the effect strength of these differences was weak (Table 4).
Table 4
Comparison of women and men in terms of the level of knowledge about the possibility of colon cancer - the Mann Whitney U test (N = 238)
| Dependent variable | Women (N = 136) | Men (N = 102) | |||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Z | p | r | |
| Level of knowledge about the possibility of colorectal cancer | 8,32 | 1,73 | 9,43 | 2,37 | -2,57 | 0,010 | -0,27 |
In the further part of the work, the age of the participants was subjected to statistical analysis in the study and it was shown that it did not significantly differentiate the level of knowledge of people visiting endoscopy departments about the possibility of CRC. Therefore, it can be concluded that the level of knowledge on this topic among people of different ages is comparable.
The study also analyzed the impact of respondents’ education on the level of knowledge about the possibility of colorectal cancer. The obtained results showed that people declaring having higher education had a better level of knowledge about colorectal cancer. Additionally, the impact of the respondents’ level of education on the knowledge of risk factors such as: genetic predispositions, the presence of polyps/adenomas in the large intestine, improper diet, intestinal inflammation, alcohol abuse, cigarette smoking, sedentary lifestyle, diabetes and insulin resistance, and treatment of colorectal cancer in the past, to the development of this cancer. The analysis of the obtained results showed that regardless of the level of declared education of the respondents, the main risk factor for developing CRC was treatment of this cancer in the past and the use of an incorrect diet. The respondents in all groups mentioned diabetes and insulin resistance the least often.
The next part of the work focused on determining what, according to respondents, are the main symptoms characteristic of colorectal cancer (it was a question with the possibility of choosing more than one answer). The most frequently mentioned symptom of CRC by the respondents was the presence of blood in the stool after defecation (83%, N=197) and a change in the nature of bowel movements (76%, N=181). More than half of the respondents identified weight loss (66%, N=157), occult bleeding (65%, N=155) and rectal bleeding (60%, N=143) as characteristic symptoms of colorectal cancer. The least frequently indicated symptoms of colorectal cancer were the feeling of incomplete evacuation (14%, N=33) and nausea (13%, N=31).
In order to determine what the knowledge of diagnostic tests for CRC was in the opinion of women and men participating in the study, a frequency analysis was performed separately in these two groups. The list of all answers and their frequency is presented in Table 5.
Table 5
The test that best diagnoses colorectal cancer in the opinion of women and men (N = 238)
Both in the group of women and in the group of men, the most frequently indicated test that best diagnoses colorectal cancer was colonoscopy, followed by a test for the presence of occult blood in the stool. In the group of women, the fewest people believed that an effective test for colorectal cancer is the CEA antigen test in the blood In the group of men, the least frequently indicated examination was proctoscopy and contrast enema.
The last part of the work analyzed the sources from which respondents most often obtained information about RJG. The data obtained are presented in Table 6.
Discussion
The analysis of the data obtained in the study showed that the level of knowledge among the inhabitants of the Lodz Voivodeship about the possibility of developing colorectal cancer was rather low. Markowska et al. [8], assessing the level of knowledge about the prevention of colorectal cancer among primary care patients in the West Pomeranian Voivodeship, revealed that the general level of knowledge about this cancer can be assessed as medium among people living in urban areas and low in rural areas. Additionally, Stefanowicz et al. [9] cite lack of participation in the screening program as the reason for the insufficient level of knowledge about colorectal cancer among people over 50. years of age.
The study analyzed whether gender was a factor significantly differentiating the level of knowledge of the inhabitants of the Lodz Voivodeship about the possibility of developing colorectal cancer. Based on the results obtained, it can be concluded that men had a significantly higher level of knowledge about the possibility of CRC occurrence compared to women. The next analysis focused on determining whether people of different ages had statistically significant differences in the level of knowledge about the possibility of CRC. The obtained results showed that age did not significantly differentiate the level of knowledge of endoscopic patients about the possibility of this cancer. Therefore, it can be concluded that the level of knowledge on this topic among people of different ages is comparable.
In a similar way, it was analyzed whether people with different education differed significantly in terms of knowledge regarding the possibility of CRC occurrence. The data obtained allowed the conclusion that the level of education was a factor that significantly differentiated the results obtained by respondents in terms of knowledge on this subject. The study revealed that people with secondary education differed statistically significantly from people with higher education in terms of the level of knowledge about the possibility of CRC occurrence. Respondents with vocational education obtained significantly higher results in this area compared to people with secondary education. There were no statistically significant differences in the analyzed range between the remaining groups.
Next, it was analyzed what risk factors influencing the development of this cancer were most often indicated by residents of the Lodz Voivodeship with different levels of education. Regardless of the level of education, the most frequently indicated risk factors were previous treatment for this disease and an incorrect diet. Respondents in all groups mentioned diabetes the least often and insulin resistance. King [2] states that cancer is the result of the accumulation of abnormal cells. A complex mix of lifestyle, environmental and hereditary factors are responsible for the development of cancer cells. According to scientists’ theory, most people have dormant genes that can lead to the development of cancer cells. Infection, environmental pollution or smoking can activate them. Diet is extremely important in cancer prevention. Włodarek [10] states that a diet rich in vegetables and fruits reduces the risk of cancer. They should be consumed in an amount of at least 400g a day in 5 portions, of which one portion may be a glass of juice. Moreover, it is recommended to limit the consumption of meat, especially red meat and processed meat products. According to research, excessive consumption of red meat increases the risk of colon cancer. Lange et al. [11] indicate a relationship between the occurrence of CRC and fat consumption. Experimental studies positively verify the hypothesis that the consumption of polyunsaturated omega 3 fatty acids reduces the risk of this cancer, while the consumption of polyunsaturated omega 6 fatty acids may contribute to the development of this cancer.
The next section focuses on determining the main symptoms characteristic of this cancer. The most frequently mentioned symptom characteristic of CRC was the presence of blood in the stool after defecation. A slightly smaller percentage of respondents also indicated a change in the nature of bowel movements as characteristic symptoms. The least frequently indicated symptoms of CRC were nausea and the feeling of incomplete evacuation. According to a study conducted on 55 patients with colorectal cancer by Nowaczyk et al. [12], rectal bleeding and a change in bowel habits (loose stools and an increase in the number of defecation) are among the symptoms of a high risk of developing CRC. Kobylańska [13] listed the key factors in the development of this type of cancer. These included age and improper diet. This cancer most often affects people over 50 years of age. Inadequate diet is responsible for 70% of cases of this type of cancer. This emphasizes the important role of nutrition in the prevention of CRC. As mentioned, excessive consumption of red and processed meat is a factor contributing to its development. Alcohol consumed in excess also contributes to many serious diseases, including cancer. Smoking and a sedentary lifestyle are also considered risk factors. In turn, people diagnosed with CRC should switch to an easily digestible diet. In 2020, Lewandowski et al. [14] conducted a study aimed at assessing awareness and general knowledge about CRC. It was conducted using an online survey form on a group of 150 people aged 17 to 68. One of the issues concerned the symptoms of this disease. The answer most frequently given by respondents was the presence of blood and/or clots in the stool.
Referring to the knowledge of diagnostic tests for CRC, both in the group of women and in the group of men, the most frequently indicated test that best diagnosed this cancer was colonoscopy, followed by a test for the presence of occult blood in the stool. Siepsiak et al. [15] believe that CRC prevention is based on applying the principles of a healthy lifestyle and undergoing screening tests. Based on the literature analysis, the most valuable such test is colonoscopy. Thanks to this examination, the doctor can detect changes and quickly initiate treatment. It can also be said that colonoscopy is a test that can save the life of a person suffering from CRC. A study conducted in 2015 [16] showed that screening tests are more available to people living in large urban agglomerations than in small towns and villages.
Stefanowicz et al. [9] stated that CRC prevention is mainly based on the elimination of risk factors and screening tests. It is worth mentioning that nowadays preoperative radiotherapy is more often used instead of the previously used postoperative radiotherapy. This was influenced by randomized trials described by Bujko [17]. They demonstrated the advantage of the currently used form of radiotherapy. Compared to postoperative irradiation, preoperative irradiation is more effective in reducing the rate of local recurrence, as well as lower both early and late toxicity, mainly in the small intestine. In the case of postoperative irradiation, the small intestine fills the dead space left by the excised tissues.
The study also analyzed the sources from which respondents most often obtained information about RJG. The vast majority of respondents become acquainted with this knowledge through internet forums and blogs. A large number of respondents use the Internet and seek medical advice on this matter. Lewandowski et al. [14] state that early detection of CRC is a fundamental condition for effective treatment. It is also necessary to emphasize the enormous role of knowledge and awareness of the population regarding the symptoms and detection of this cancer. It has been shown that a higher level of knowledge in the field of CRC increases the likelihood of undergoing tests that can detect this disease.
Conclusions
The level of knowledge of the inhabitants of the Lodz Voivodeship about the possibility of CRC occurrence was low.
Previous treatment with CRC and an incorrect diet were considered by the respondents as the key risk factors for this cancer.
Men had a significantly higher level of knowledge about the possibility of CRC occurrence compared to women.
According to respondents, the main symptoms of colorectal cancer were the presence of blood in the stool after defecation and a change in the nature of bowel movements.
People with primary education had a significantly lower belief in the impact of inflammatory bowel diseases on the development of CRC than people with secondary, vocational and higher education.
The most frequently indicated test for the best diagnosis of CRC (both in the group of women and in the group of men) was colonoscopy and testing for the presence of occult blood in the stool.
In the opinion of respondents, internet forums/blogs, the Internet and doctors are the main sources of information about CRC.








