

 POLSKI
POLSKI







Introduction
Osmotic homeostasis and water balance are mainly regulated by thirst and antidiuretic hormone (ADH). Under physiological conditions, secretion of ADH depends on the serum osmolality and arterial blood volume [1]. Furthermore, non-osmotic stimuli of ADH release include haemodynamic changes, stress, and hypoxia [2]. The effective osmolality of the extracellular fluid (ECF) is significantly influenced by sodium concentration. Hyponatraemia, defined as sodium concentration below 135 mmol/l, is one of the most common electrolyte imbalances. The aetiology of true, hypotonic hyponatraemia is classified according to the state of the volaemia (hypovolaemic, euvolaemic, or hypervolaemic). The symptoms depend on the severity of the hyponatraemia and the rate of decrease of sodium [3]. Acute, profound hyponatraemia causes a rapid fluid shift from ECF to intracellular fluid, which can lead to cerebral oedema. Urgent diagnosis of the cause of hyponatraemia, as well as immediate initiation of appropriate causative treatment, which varies slightly depending on the aetiology of hyponatraemia, is of key importance. We report our own experience based on 3 cases of transient severe hyponatraemia (<125 mmol/l) in previously healthy children diagnosed between 2020 and 2021 as well as a literature review of polydipsia-hyponatraemia syndrome. In all cases hyponatraemia resolved completely and without any sequalae.
Clinical descriptions
A summary of laboratory values of children upon admission to the Emergency Department is presented in Table I.
Table I
Summary of laboratory values upon admission to the Emergency Department
case 1
A 2-year-old boy, with no past medical history, was admitted to the Emergency Department after an episode of seizures with respiratory failure. Laboratory tests revealed hyponatraemia: 120 mmol/l, plasma osmolality 243.6 mOsm/kg H2O (normal range 275–295), and with potassium concentration in normal range. Computed tomography (CT) of the central nervous system did not show any abnormalities. There was no information about treatment at that time. He was transferred to the Paediatric Intensive Care Unit (PICU). Two hours later, a physical examination showed slight signs of dehydration (sunken eyes). Hyponatraemia (129 mmol/l) was still present. During this the time fluid and electrolyte deficiencies were compensated continuously with balanced crystalloid solution. Moreover, he was given dexamethasone (no information about dosage regimen). As a result of the treatment, for 8 hours, his sodium concentration increased by 23 mmol/l, so the correction of hyponatraemia was too aggressive. Further observation in the PICU revealed that the child had polyuria (4,000 ml of urine/18 hours). Therefore, he was treated with 0.5 mcg of desmopressin intravenously twice a day (start 16 hours after admission when the sodium concentration was 139 mmol/l). During the first 2 days of hospitalisation in the PICU, the child was still intubated, with blood pressure (BP) that required stabilisation with the infusion of norepinephrine (0.15 µg/kg/min). Due to suspicion of aspiration pneumonia, antibiotic treatment was initiated. Magnetic resonance imaging (MRI) of the head revealed no clinically significant abnormalities. After 4 days, the child was transferred to the Department of Paediatric Endocrinology (DPE) for further diagnosis. Dexamethasone was not administered, and desmopressin therapy was discontinued. The plasma sodium concentration was within the reference ranges (from 144 to 138 mmol/l), but from the first days of observation at DPE, polydipsia and polyuria were present (on the seventh day: the patient drank 6.5 l/m2 and urinated 5.4 l/m2 a day). His mother confirmed that the same was happening at home, before the hospitalisation, and she was giving him mainly spring water with a low concentration of minerals. Therefore, a dehydration test was started in the ninth day of hospitalisation and it was inconclusive (Table II). It seems that the patient could be overhydrated at the onset of dehydration test as he had relatively low plasma osmolality both at the beginning and at the end of the test, and a very small increase of plasma osmolality during the test was observed. In such situation a more than 3% decrease of weight might be related only to losing the excess of water and thus insufficient to cause the increase of AVP secretion. On the 10th day of observation, the patient urinated less: 2.1 l/m2/24 hours.
Table II
Results of dehydration test for the case 1
case 2
A 20-month-old girl was admitted to the paediatric ward on the first day of the disease, manifested by fever up to 39.3°C, due to refusal of fluid intake and deterioration of general condition. On admission, she was in a moderately severe general condition, apathetic, drowsy. The physical examination revealed: pupils lazily reacting to light, reddened throat, drying oral mucosa, but high blood pressure (123/73 mmHg), her weight was 10 kg. A balanced crystalloid solution (150 ml/2 h) and antibiotic therapy (amoxicillin + clavulanic acid) were administered. More than an hour after admission, the child’s neurological condition deteriorated further. Laboratory tests before starting fluid therapy revealed hypotonic hyponatraemia: sodium 121 mmol/l, plasma osmolality 252 mOsm/kg H2O (normal range 275–295). Complete blood count, inflammatory marker concentrations, and urine analysis were normal (urine specific gravity: 1.02 g/ml, normal range: 1.016–1.022). The fluid administrated was changed to 0.9% NaCl (250 ml/2 h); in addition, dexamethasone was used (4 mg), followed by an infusion of 3% NaCl (20 ml/h). The child’s condition improved. Due to the excessively rapid increase in sodium (13 mmol/l/6 hours), 3% NaCl was discontinued, and an infusion of isotonic fluid was ordered (250 ml/2 h). Eight hours after admission to the hospital, due to the good general condition of the girl, the intravenous fluid therapy was stopped. An in-depth history of the patient revealed that the girl had recently (probably due to the hot summer) consumed an average of 9.5 l/m2 of fluids a day, mainly spring water. In the following days, no fever was observed. In laboratory tests the concentration of electrolytes was normal, but urine gravity decreased to < 1.005 (normal range: 1.016–1.022) with low urinary sodium excretion (< 20 mmol/l). The patient urinated 3.6 l/m2 and drank 4.3 l/m2 a day. The girl was transferred to the DPE on the 5th day of observation. On admission, general condition was assessed as good, only short stature was noted (height SDS: –2.03). The plasma sodium concentration was in normal range (Na 140 mmol/l) but polydipsia (from 2.2 to 3.2 l/m2/day) and polyuria (from 2.3 to 3.2 l/m2/day) were still observed. So, a dehydration test was started on the 9th day of medical observation, during which the patient did not urinate from 6:00 to 12:00, and as so the test was aborted. MRI of the pituitary gland revealed a small cyst between anterior and posterior lobe of the pituitary (no clinical significance). At the age of 3.5 years a diagnosis of short stature was continued: growth hormone deficiency was excluded [4]. The child’s target height was calculated to be 156 cm (target height SDS: –1.66), so this may speak for familial short stature.
case 3
A 5-month-old boy with no past medical history was admitted to the Emergency Department after an episode of right-hand tremor and lividity. The patient was born in the 41st week of pregnancy, with a body weight of 3120 g, and 10 points on the Apgar score. He was fed with infant formula (160–180 ml of the formula 5–6 times a day). Moreover, according to the parents’ reports, the boy drank a lot a few days before admission. The past medical history of this boy was unremarkable. Due to respiratory tract infection for 2 days before admission he was receiving amoxicillin with clavulanic acid and nebulisation with fenoterol, ipratropium bromide, and budesonide. In the emergency room, he was in a serious condition, with right-sided convulsions and saturation of 87%. Diazepam was administrated. Blood gas analysis showed mixed metabolic and respiratory acidosis, together with hyperglycaemia 292 mg/dl and hypotonic hyponatraemia: sodium 113 mmol/l (corrected Na 116 mmol/l), and plasma osmolality 243.6 mOsm/kg H2O (normal range 275–295). He received 350 ml of 0.9% NaCl during the next hours and 0.4 U/h of insulin. The child was then transferred to the PICU when high blood pressure was noticed. Insulin therapy was stopped, and hyponatraemia (Na 117 mmol/l) was corrected by 3% NaCl (amount unknown). Eighteen hours after admission to the hospital the intravenous fluid therapy was stopped (Na 136 mmol/l). Six hours after stopping the administration of 3% NaCl, the development of profuse diuresis and hypernatraemia was observed (about 200 ml/kg/24 hours, throughout the second day sodium was from 151 to 159 mmol/l, serum osmolality from 307 to 324 mOsm/kg H2O). Diabetes insipidus (DI) was suspected due to polyuria, and hypernatraemia and desmopressin were administered with the effect of resolving polyuria and normalising sodium levels. MRI of the head and pituitary gland was performed, in which the expected signal the posterior pituitary gland (“bright spot”) was missing. Administration of desmopressin was continued initially intravenously, then orally in various doses from 3.75 to 7.5 µg/dose and at variable times under the control of fluid balance. Despite repeated attempts, it was not possible to establish a fixed dose and timing of drug administration due to the high variability of diuresis. Initially, the boy required higher and more frequent doses of desmopressin, then a clearly reduced demand for desmopressin was observed, and in the last 2 days of his stay he received a single dose of 3.75 µg but maintaining the proper state of hydration. The boy was transferred to the DPE on the 19th day of observation for further diagnosis. Desmopressin therapy was discontinued, but the fluid balance was maintained and daily urine amount was 1.4 l/m2/24 hours. Sodium levels, glycaemic profiles, and HbA1c were within reference ranges.
Our patients’ sodium concentration and treatment on the first day of hyponatraemia are summarised in Figure 1. The amount and type of fluids given to Patient 1 on the first day of hospitalisation are unfortunately not available. Adrenal insufficiency and hypothyroidism were all excluded. Assessment of kidney and liver functions was unremarkable. The results of hormonal tests of our 3 patients are presented in Table III. All patients were discharged home without any pharmacological treatment. During the next follow-up visits, general condition of all children was good, the plasma sodium concentration as well as serum and urine osmolality were within the reference ranges.
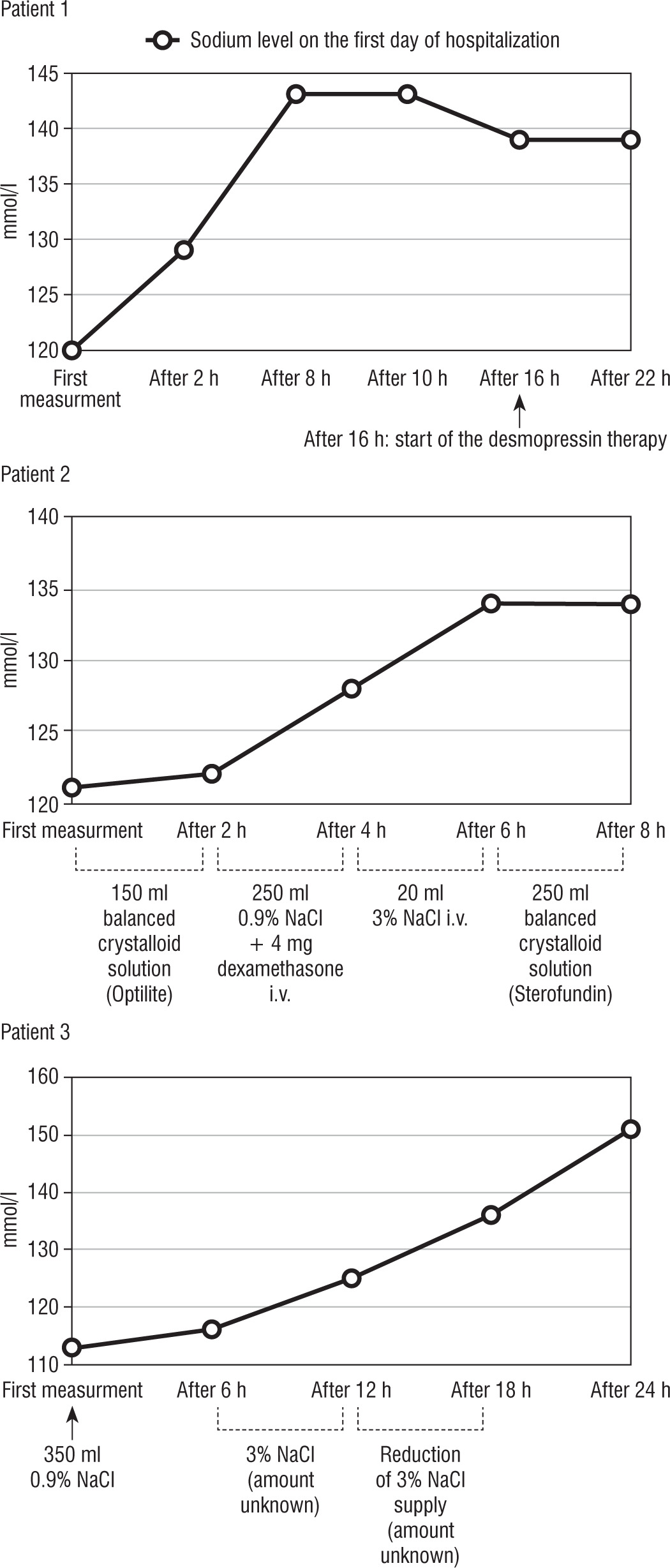
Table III
Summary of laboratory values upon admission to the Emergency Department
An informed consent for publication of case reports was given by all the legal guardians of children.
Discussion
Hypotonic hyponatraemia (plasma osmolality < 275 mOsm/kg H2O) is the most common form of hyponatraemia and is divided depending on the patient’s hydration status into the following:
hypovolaemic hyponatraemia, in which there is a loss of both sodium and water, which can pass through the skin, the digestive tract, or kidneys (diuretics, mineralocorticoid deficiency tubulopathies, or cerebral salt-wasting syndrome),
euvolaemic hyponatraemia, which might be caused by syndrome of inappropriate antidiuretic hormone secretion (SIADH), as well as primary polydipsia (PP), glucocorticoid deficiency as part of secondary adrenal insufficiency or long-term sodium-poor diet,
hypervolaemic hyponatraemia, in which there is an increased secretion of vasopressin due to relative reduction of the effective intravascular volume (chronic heart failure, cirrhosis, nephrotic syndrome) or caused by an excessive supply of non-electrolyte fluids, when the excretion of the kidneys is impaired (advanced chronic kidney disease) [3].
In our cases the children were thoroughly investigated at their initial presentation; the work-up was done after the introduction of multipronged therapeutic approaches. The physical examination in terms of volaemia was not adequately described, and urine osmolality was not determined – both of these parameters are obligatory in the initial evaluation of a hyponatraemic subject. Acute water intoxication could be considered in a patient with euvolaemic hyponatraemia when urine osmolality is <100 mOsm/kg/H2O.
In all the 3 cases hyponatraemia would have been multifactorial, including a component of SIADH or inefficient renal water handling.
Polydipsia-hyponatraemia syndrome, the condition in which polydipsia results in hyponatraemia, occurs in 5% to 10% of patients with PP [5]. Long-term physiological changes connecting with overhydration are not fully understood. When consumption exceeds the excretory capacity of the kidneys, which is estimated as a maximum of 12 l/day [6] or when the excretory capacity of the kidneys is reduced, the excess of free water supply is not excreted, and results in hyponatraemia. Several risk factors contribute to the occurrence of hyponatraemia as a result of self-induced water intoxication, such as acute consumption of a large amount of fluids in a short period and intake of low-sodium fluids [7]. Osmotic dysregulation and SIADH have also been reported in polydipsic patients [5]. The lower osmotic threshold for ADH secretion and the impairment in urinary dilution after water loading, presumably due to greater sensitivity to ADH of the renal tubule collecting duct or a vasopressin-independent defect caused by damage to the genitourinary system, in psychotic patients with polydipsia and hyponatraemia, compared to cases with polydipsia only, were found [8]. Although in overhydration, a physiological suppression of ADH and maximally suppressed urine osmolality are observed, in PP patients, a certain amount of ADH is needed to develop hyponatraemia. It has been shown that patients with PP and hyponatraemia have a higher urine osmolality than patients with PP who remain normonatraemic [9]. Therefore, conditions favouring ADH secretion (some medications or a stress as a non-osmotic stimulator of ADH) can cause a rapid decrease in serum sodium levels.
In the second case, SIADH should be considered, in which increased secretion of vasopressin and/or increased sensitivity to ADH causes increased water retention, resulting in hyponatraemia and inappropriate high urine osmolality, but not in polyuria.
Maybe earlier overhydration (the girl consumed an average of 9.5 l/m2 of fluids a day) can lead to the lower osmotic threshold for vasopressin and/or greater sensitivity of renal tubules for ADH so the conditions favouring ADH secretion (such as the girl’s infection with elevated body temperature and accompanying sudden refusal to drink fluids) could have contributed to development SIADH and caused profound hyponatraemia. This would explain why the girl, with a serum sodium concentration of 121 mmol/l, initially had normal urine specific gravity. Unfortunately, urine osmolality was not determined, but a good correlation between the specific gravity and the osmolality of a urine sample is observed, obviously after exclusion of glycosuria, albuminuria and hypercreatininemia [10]. The influence of the existing infection, mainly pneumonia, in children on the development of SIADH was noted [11]. The frequent procedure during an infection is to increase fluid ingesting as a prevention of dehydration. One, however, should remember about the possibility of inducing water poisoning in a patient consuming excessive amounts of hypotonic fluids, especially when exposed to non-osmotic ADH stimulus, such as an acute infection or stress, and/or reduced renal excretory capacity. However in the case of SIADH, the treatment of hyponatraemia involves limitation of fluid intake. In our case, fluid therapy not only did not worsen the hyponatraemia, but even corrected it. An argument in favour of diagnosis of PP or inefficient renal water handling as the cause of hyponatraemia is that the parents reported that their children had been drinking large amounts of low-sodium spring water a day during an unspecified period. Polydipsia and polyuria was observed in all our patients at home and was assessed retrospectively and subjectively. After admission to the hospital, an accurate fluid balance was carried out and polyuria was still observed after normalization of fluid intake. Severe, true hyponatraemia in patients causes a decline of serum osmolality, which in turn results in ADH suppression. This, together with the reversal of non-osmotic stimuli of ADH secretion, can result in free water diuresis and a rapid increase of serum sodium level if fluid intake is restricted [12]. This mechanism may explain the clinical course of hyponatraemia in our patients, i.e. rapid overcorrection of sodium concentration and a presence of polyuria observed during the first days of hospitalization, followed by normalization of urine output [13]. The observed rapid sodium increase connected with high blood pressure and followed by increased diuresis could be also be related to too aggressive fluid administration. Unfortunately, complete data on fluid balance was not provided in all cases. Hypovolemia excludes the diagnosis of SIADH as well as PP, but the sensitivity and specificity of clinical assessments of hydraTreatment of severe symptomatic hyponatraemia with 3% hypertonic saline is recommended,with the immediate goal of upraising serum sodium concentration by 4–6 mmol/l. Subsequently, it is suggested that in the chronic hyponatraemia the serum sodium concentration should not increase more than 8–10 mmol/l in total over the first 24 hours of the treatment, in order to minimize the risk of osmotic demyelination syndrome [1, 3, 14]. Hyponatraemia is a contraindication to the administration of desmopressin. The only situation where the treatment with desmopressin in hyponatraemia might be beneficial, is the simultaneous administration of desmopressin with 3% hypertonic saline to prevent too rapid correction of sodium levels [15]. This technique might be applied to our patients whose sodium levels were corrected too quickly in accordance with the current guidelines. The only presence of polyuria does not entitle to diagnose arginine vasopressin deficiency (AVP-D). After the normalization of serum sodium, increased diuresis was observed, therefore a dehydration test was performed. The diagnostic standard to distinguish PP from AVP-D is the dehydration test, but sometimes the interpretation of the tests is much more complicated. In the chronic condition of overhydration (> 3 days), a sustained physiological suppression of ADH results in the downregulation of Aquaporin-2 water channel in the kidney collecting duct, which ends with a transient (up to 5 days) inability to concentrate urine in response to ADH stimulation [14]. Another mechanism worth mentioning is washout of the medullary gradient from persistent PP [16]. It has been suggested that the presence of hypernatremia and/or high osmolality before dehydration test in patients with polydipsia is indicative of AVP-D and hyponatremia and low plasma osmolality is indicative of PP [17]. No signal from the posterior pituitary gland was considered typical of patients with AVP-D in brain MRI. The “bright spot” or area of hyperintensity seen in normal T1-weighted images on MRI is the result of T1-shortening effects of ADH, which is stored in the posterior lobe of the pituitary gland [18]. However, later there were reports of patients with persistent area of hyperintensity despite diagnosed AVP-D [19]. Similarly, another study showed that the bright spot was persistent in 36% of AVP-D patients, while it was missing in 36% of PP patients [20]. Therefore, the absence of the bright spot in MRI is not sufficient evidence for the existence of AVP-D, as it can also occur in patients with confirmed PP, and even in healthy people [21].
Conclusions
While diagnosing hyponatraemia, it is of major importance to carefully ask in the anamnesis about habits related to the amount of urination and fluid intake and the type of consumed fluids. It should also be noted that a frequent procedure during an infection is to increase fluid ingesting as a prevention of dehydration, the negative effects of which are known. One, however, should remember about the possibility of inducing water poisoning in a patient consuming excessive amounts of hypotonic fluids, especially when exposed to non-osmotic antidiuretic hormone stimulus, such as an acute infection or stress, and/or reduced renal excretory capacity. The presence of only polyuria does not justify a diagnosis of arginine vasopressin deficiency (AVP-D), and especially the implementation of desmopressin treatment before all diagnostic procedures are completed, specifically in the case of hyponatraemia. Desmopressin can be used simultaneously with intravenous 3% saline solution in the treatment of very severe hyponatraemia, only to avoid overcorrection of natraemia. In patients after profound hyponatraemia polyuria could be observed after normalisation of fluid intake, but it is temporary.