
Introduction
Currently, an observable phenomenon in society is the lack of time and the pursuit of material things, which ultimately leads to negative impacts on the population’s health. People live at an alarmingly fast pace, get exposed to environmental pollution, and consume highly processed food. They lack the time and willingness to do the right amount of physical activity or exercise. They experience stress, which they cannot always cope with in healthy ways. They may also encounter a lack of support from their relatives, which additionally contributes to the emergence of poor relations and negative emotions. In this way, the risk factors for diseases amplify, favoring the occurrence of various diseases. One of these types of diseases, whose incidence and prevalence is increasingly noticeable in modern times, is inflammatory bowel diseases (IBD), which include Crohn’s disease (CD), ulcerative colitis (UC) and other mixed or unspecified intestinal diseases. IBD is a group of chronic diseases of the digestive system with periods of exacerbation and remission. Their exact etiology is completely unknown, though it is believed that the development of IBD is influenced by genetic factors, environmental factors as well as immune disorders (1). The highest incidence is observed in highly developed countries, such as the countries of Western Europe or North America. The incidence of these diseases is increasing in Poland. The most likely reason for this observation is the development of diagnostic methods and lifestyle changes due to modernization (2,3). Mostly young people aged 20-40 are ill, although more people are diagnosed with it in the range of 15-35 years. CD belongs to the group of incurable diseases, and therefore, after diagnosis, the patient must manage the disease for the rest of their lives. They face many burdens and morbidities related to the disease, which reduces their quality of life (4).
The aim of the study is to assess the quality of life of people diagnosed with CD and to analyze the factors that have a significant impact on their level of life satisfaction.
Material and methods
The research group consisted of 100 patients diagnosed with CD in the period from December 2022 until May 2023 The patients were looked after by the Specialist Gastroenterological Outpatient Clinic in Lodz. During the visit to the Clinic, patients were asked to fill in the questionnaire, for which they gave their informed consent. Patients were informed that participation in the study was voluntary and anonymous. They were provided with additional information on the rules for completing the questionnaire. The study was conducted with the consent of the local Bioethics Committee and in accordance with the principles of the Declaration of Helsinki. The study was conducted using the diagnostic survey method, including the Life Satisfaction Scale (SWLS) and a self-authored questionnaire. For the assessment of life satisfaction, the SWLS scale was used, which contains 5 statements assessing the degree of life satisfaction relating to the respondent’s life so far. The result of the measurement was the overall level of satisfaction with life. The scale is designed to test healthy and sick people. The respondent indicates to what extent he agrees with each statement. The instruction explains the meaning of individual answers, which mean: 1 - I disagree completely, 2 - I disagree, 3 - I rather disagree, 4 - I neither agree nor disagree, 5 -I rather agree, 6 - I agree, 7 - I completely agree. The grades are added up and the overall score is the degree of satisfaction with one’s own life. The range of results is between 5 and 35 points. The higher the score, the greater the sense of satisfaction with life. The test result can be compared with the mean results of the appropriate groups of healthy or sick people and converted into standardized units. The interpretation of the result follow the properties characterizing the sten scale. The results within 1-4 of the sten were considered low, and 7-10 as high, which corresponds to the area of about 33% of the lowest results and the same number of the highest scores in the scale. The results within 5 and 6 sten were considered average (5). The proprietary questionnaire contained 16 closed and 2 open questions, which concerned demographic variables, family situation and the need for education and support in illness. Statistical analysis was performed using the SPSS Statistics 21.0 statistical package. The ANOVA test (analysis of variance) was used to test the statistical relationship between the analyzed features. A 5% risk of inference error was assumed. A probability value of p <0.05 was considered statistically significant. The analysis of variance (ANOVA) for a single classification examines the effect of one classifying factor (divided into many levels) on the values of the measured measurable feature.
Results
The group of 100 respondents were people with confirmed CD. The detailed characteristics of the study group are presented in Table 1.
Table 1
Characteristics of the studied group
Most of the surveyed respondents 55% (n = 55) were educated in the field of their disease by a specialist doctor. A slightly smaller number of respondents 19% (n = 19) named a specialist doctor and a nurse as their educator. Every tenth patient, 10% (n = 10) indicated a nurse as the only educator of their illness, and some 6% (n = 6) were not educated about the disease at all. A vast group of respondents 96% (n = 96) admitted in the study that in difficult times of illness they obtained support from medical personnel. It was most often informational support 32% (n = 32) and emotional support 31% (n = 31), and 16% of patients decided that they did not need support in their illness. Also, the vast majority of the respondents 84% (n = 84) did not declare belonging to any support group. The research conducted on 100 randomly selected patients with CD allowed to assess their level of satisfaction with life. The average number of points obtained by the respondents was 19.33, with a standard deviation of 4.86, which means that they experience an average level of quality of life (Tab. 2).
Table 2
General level of satisfaction with life
| STEN | M | SD | N | % |
|---|---|---|---|---|
| 1 | 6,00 | 0,99 | 2 | 2 |
| 2 | 10,00 | 0,33 | 2 | 2 |
| 3 | 12,79 | 0,08 | 14 | 14 |
| 4 | 16,07 | 0,36 | 14 | 14 |
| 5 | 19,00 | 0,85 | 27 | 27 |
| 6 | 22,32 | 0,71 | 19 | 19 |
| 7 | 24,81 | 0,81 | 16 | 16 |
| 8 | 27,17 | 0,73 | 6 | 6 |
| 9 | 0,00 | 0,00 | 0 | 0 |
| 10 | 0,00 | 0,00 | 0 | 0 |
| Wskaźnik ogólny | 19,33 | 4,86 | 100 | 100 |
Interpreting the results presented in Table 3, it can be concluded that the number of patients declaring an average level of life satisfaction is less than 50% of the cohort. A large group of respondents (32%, n=32) said they were in judge their life satisfaction as a low quality of life.
Table 3
SWLS scale - Level of life satisfaction
| Poziom satysfakcji z życia | Number of respondents |
|---|---|
| Wysoki (7-10) | 22 |
| Przeciętny (5-6) | 46 |
| Niski (1-4) | 32 |
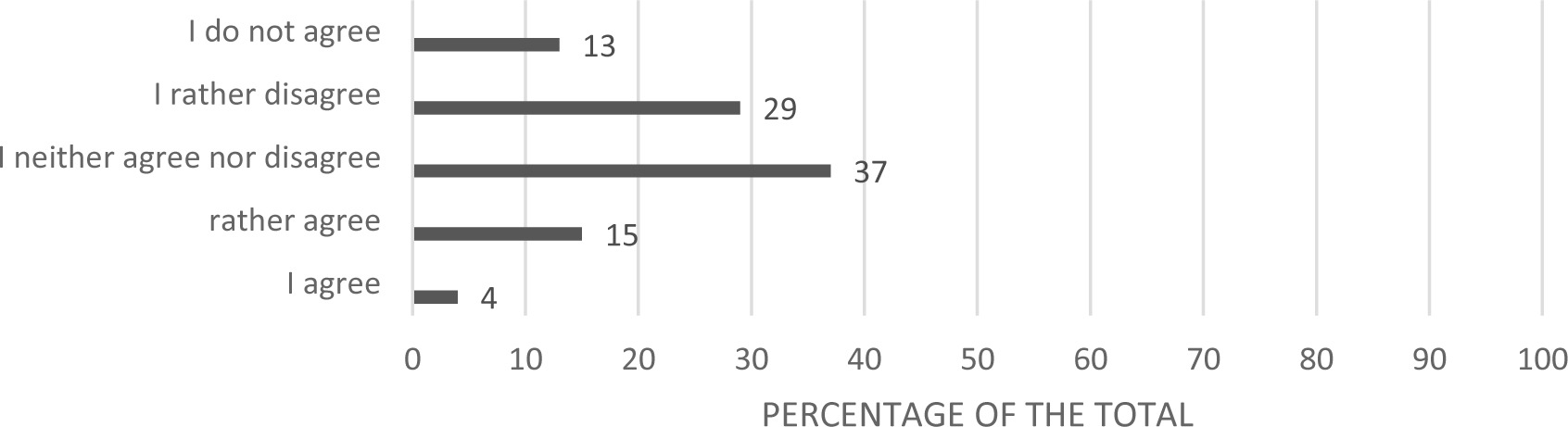
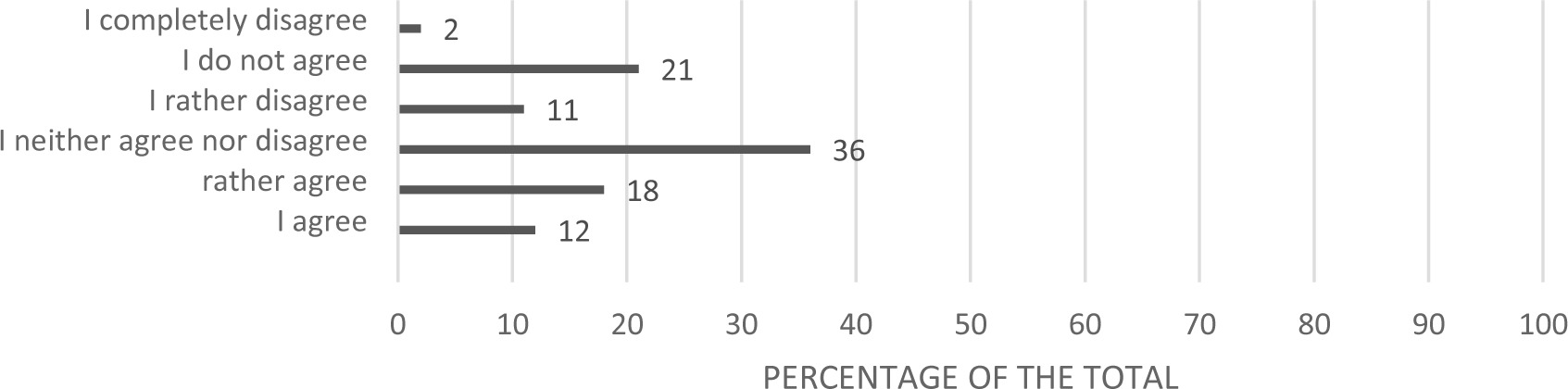
The statistical analysis of the SWLS scale showed that it is difficult for people taking part in the study to determine how accurately they perceive their life. Detailed data is presented in Figures 1, 2, 3.


The statistical analysis of the SWLS scale also showed that every fifth respondent (21%, n = 21), did not achieve what is most important to him in his life, and again, every fifth respondent (22%, n=22) identified that if he had the chance to live life again, he would make some changes. The above description is presented graphically in Figures 4 and 5.

Statistical calculations from the conducted study show that demographic factors such as: gender, age, education level, place of residence, as well as professional status, type of work, financial situation, having children and contact with family do not affect the level of life satisfaction in the group of patients with CD. On the other hand, the study showed a significant correlation between education about the disease and the quality of life of the respondents. People who were educated about the disease showed a higher level of life satisfaction (Table 4).
Discussion
CD is a chronic inflammatory disease process that can occur anywhere in the digestive system. This disease is characterized by alternating periods of exacerbation and remission (6). Inflammatory changes are most often localized in different sections of the small intestine. This disease mainly affects young people. During the course of the disease patients may suffer from numerous ailments that negatively affect everyday functioning (7,8). These include: loose, high-frequency stools (with an admixture of blood or mucus), abdominal pain, fever, weakness, symptoms related to extraintestinal manifestations of the disease or mental discomfort (9,10). The patient must reorganize his or her life so that it is possible to reconcile professional and social activity with the symptoms of the disease. Very often, diagnosing CD can be challenging. It takes patience and time to make an accurate diagnosis as well as a treatment plan that controls the disease. Well-targeted treatment improves the patient’s well-being, reduces negative ailments, and allows him to live to some extent as before the diagnosis of the disease (11,12).
The quality of life deteriorates in people who struggle with CD and experience severe gastrointestinal symptoms. In the conducted research, the majority of respondents assessed the level of life satisfaction as average (5-6 sten) - 46 people. Similar results were obtained by ZielińskaWięczkowska et al. in studies carried out in two hospitals in Bydgoszcz. The average results also prevailed among the respondents (13). Glińska et al. demonstrated that the overall average life satisfaction index for all respondents reached the lower limit of the average life satisfaction (14). Perek presents a different opinion, because he proves that the respondents declared a relatively good quality of life. Additionally, he claims that the disease does not have a significant impact on the quality of life (15). In our research, the overall disease was taken into account, without dividing it into periods of exacerbation and remission. Bąk E. et al. in their work proved that patients in remission reported very good or good quality of life, while bad or very bad quality of life was reported in patients during exacerbations (5).
The paper analyzes demographic factors and their impact on the level of life satisfaction. Consideration was given to gender, age, education, place of residence. Statistical analysis did not show any correlation between the above-mentioned factors and quality of life. In the literature, the lowest life satisfaction was more often reported by women, people living in the countryside and people with low education. People with CD feel less attractive, have difficulties with running a family, social and professional life. People living in the countryside have limited access to medical services and support organizations (14).
Another issue taken into account in the own research was the professional status and the type of work performed. After an in-depth analysis, no correlation was found between these factors and the level of life satisfaction. However, when reviewing the literature, people with CD, compared to the general population, show reduced professional activity and fewer professional achievements, which reduces their quality of life. According to Chrobak-Bień, the occurrence of periods of exacerbations and remissions contributes to more frequent visits to the hospital, which is related to with absence from work or with the need to retrain and change the nature of work (17). Chronically ill people who live with family members or have children are more likely to receive help from their loved ones. In periods of exacerbation of the disease, they can depend on social, emotional, financial and information support. They know that they can rely on their family in a difficult situation. Rachubińska et al. confirm that the support of friends and family has a positive effect on improving the quality of life of patients with CD (18). The presence of the family in the place of residence contributes to the improvement of life satisfaction. Nevertheless, the statistical analysis of own research did not show any significant correlation between having children or sharing a flat with family members with the level of life satisfaction. Another issue analyzed in the authors’ own research was the subjective assessment of contact with the family. According to the collected data, there is no correlation between the examined factor and the level of life satisfaction. In the literature on the subject, there is documentation on the positive impact of good contact with family and friends on patient life satisfaction. Support in such situations strengthens the patient’s will to fight stressful events. Then such a person may feel loved and needed (19). Miklas et al. pointed out that the deterioration of relations with a partner caused by intestinal problems negatively affects the sexual sphere of women struggling with IBD. Due to bothersome symptoms, the patients noticed that they were sexually cold, which distanced their partners from each other (20).
Our own research also considered the influence of the financial situation of the respondents on the level of life satisfaction of patients with CD. Statistical analysis showed no relationship between these factors. By reviewing the literature, however, it is possible to find information to link the financial situation with the quality of life. Reportedly, older people show higher levels of life satisfaction than younger people. This may be related to a more stabilized financial situation and professional status of these people (21).
A critical factor which should be taken into account in the conducted studies is the education of patients with CD. Links were sought between education among patients and the level of life satisfaction. Statistical analysis showed a significant relationship between education about the disease and the level of quality of life. People who have been educated about the disease show a higher level of life satisfaction. This is because these patients are more aware of their disease. They pay more attention to various issues of everyday life that affect their well-being. Education should focus on promoting physical activity, using a balanced diet, and quitting smoking as this may exacerbate the disease (22). This is confirmed by the research conducted by Perek M., Cepuch G. et al. according to which educated youth were sufficiently informed about the situation that concerned them. The knowledge gaps among the respondents were not large, which was related to effectively conducted education. (15). In turn, being aware of the disease and its limitations allows you to appreciate the smallest things and enjoy life. The author’s research also included the influence of the educator on the quality of life of patients. There was no positive correlation between the examined factors. On the other hand in the literature there are reports to the contrary. The educational role of the nurse was found to be medically crucial and positively influenced the patient’s sense of quality of life. The aim of the study was to understand and evaluate the impact of specialist nursing interventions on the improvement of care for gastroenterological patients. Studies have shown a better mental well-being of these patients, which is associated with the feeling of peace and relief (15).
The fact that this chronic disease requires reorganization of one’s life so far arouses negative emotions in patients. The sick are afraid of what tomorrow will bring. Sometimes they face difficult choices regarding their financial and professional situation. Due to the specificity of the disease, they cannot perform the professions they have chosen or dreamed of. The negative emotions associated with it burden their psyche. They can also become depressed. In order to remedy this, various organizations are created to support people in such situations. At such meetings, there are people who experience the same problems as them. Ties are formed and their reality is not as terrible as it previously seemed. As such, the support at CD is a very important component of their comprehensive care. During their stay in the hospital, after diagnosis, medical personnel should encourage patients to seek support groups and actively participate in them, as well as provide support in medical facilities. Better physical and mental well-being leads to faster and longer remission of the disease, increases the level of adaptation to a given situation and acceptance of the disease, which is associated with an improvement in the quality of life. The literature supports that patients who belonged to support groups showed a higher level of life satisfaction than those who coped with the disease on their own and did not use the help of others (14). On the other hand, the authors’ own research did not prove that receiving support from medical personnel improves the level of life satisfaction. Similarly, the type of support that respondents needed did not correlate with the level of life satisfaction.
Being aware of what life with CD is associated with, we, in the medical field, should look for all ways to improve the quality of life of patients. Knowing that satisfaction with living conditions is a very important issue for maintaining good health, the task of medical staff is to educate patients about the disease, which, as our own research has shown, positively correlates with the level of life satisfaction. Due to the increase in the incidence of IBD in recent times, specialists are obliged to help patients suffering from these diseases. Nurses, being in close proximity to the patient, are in an excellent position to engage in education, support, nursing, treatment, as well as conducting research in the field of quality of life. The obtained results allow them to identify problems and deficits and adjust activities to the needs of patients. As a result, patients who received help adequate to their health condition show better life satisfaction.
Conclusions
The general level of satisfaction with the life of people with CD was at an average level. Demographic factors, ie gender, age, education level, professional status, type of work and place of residence did not affect the quality of life of people with CD. Statistical analysis of own research showed that there is no correlation between having children and the level of quality of life of people with CD. The material situation did not change the level of life satisfaction. Conducting education influenced the quality of life. People who have been educated about the disease have shown a higher level of life satisfaction. Providing support by medical staff did not contribute to improving quality of life.








